The stability of breast cancer patients when using the 6DoF couch
Jessica van der Himst,
The Netherlands
PO-1843
Abstract
The stability of breast cancer patients when using the 6DoF couch
Authors: Jessica van der Himst1, Amy de la Fuente1, Sjoerd Hoek1
1Amsterdam UMC, Radiotherapy, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
To evaluate the influence of a 6D couch
correction on the stability of breast cancer patients and whether there is a
relationship between the magnitude of pitch and roll movements and patient
stability. In addition, to assess whether there are subgroups for which the
effect of a 6D couch correction is greater and whether the stability of breast
cancer patients is comparable to lung cancer patients.
Material and Methods
The research population concerns the first 84
breast cancer patients treated between December 2020 and March 2021 on the
Radiotherapy department in VUmc. All patients are treated on a Truebeam linear
accelerator (Varian Medical Systems) and were positioned arms up in supine
position on a thoraxsupport (MacroMedics). Online registration data were
evaluated. In total this concerns 767 radiotherapy fractions. A CBCT was made
for each fraction and a verification CBCT was made when pitch and/or roll was ˃1°
(199 fractions). The CBCT’s were registered online using an automatic 6D bone
match, the ROI was placed around the sternum and thoracic wall. Thereafter, in PBI
or SIB treatments an automatic or manual 3D registration was done on the surgery clips.
Results
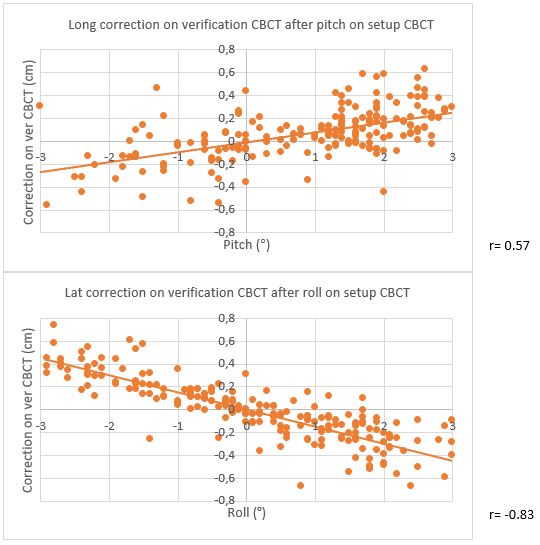
There is no
correlation between the magnitude of pitch on the setup CBCT and the magnitude
of vertical (r=-0.07) and lateral (r=0.05) corrections on the verification
CBCT, but there is a moderate correlation between pitch and the longitudinal (r=0.57)
correction. Longitudinal corrections up to 0.63 cm are required on the verification
CBCT after pitch (figure 1). Every dot shows the executed correction on the
verification CBCT. Pitch and roll data
≤1˚ also appear in the scatter plots. In the scatter plot of pitch a
verification CBCT was made because of roll >1˚ and vice versa.
Secondly, there is no correlation between roll and the magnitude of
vertical (r=-0.02) and longitudinal (r=-0.09) corrections on the verification
CBCT. However, there is a strong correlation between roll and the lateral
(r=-0.83) correction on the verification CBCT. Lateral corrections up to 0.74
cm are required (figure 1).
Except for some minor differences it appears that correlations of the subgroups
breast cancer patients correspond to those for the entire group. Subgroups were
PBI, breast FAST (+SIB), breast (+SIB), breast loco-regional, chest wall
loco-regional and axilla.
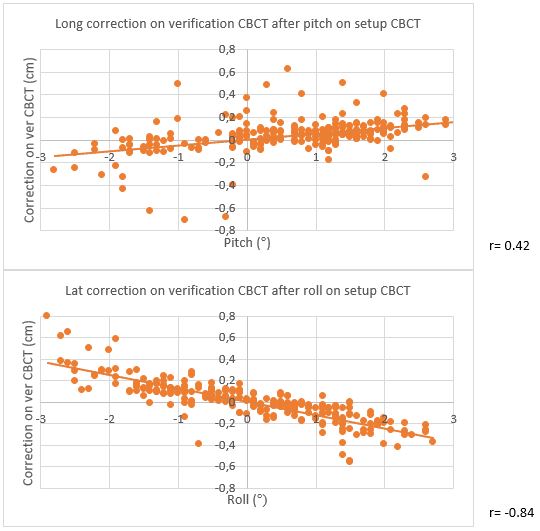
There are no significant differences in correlation coefficients between breast
and lung cancer patients (figure 2).
Conclusion
After performing
pitch and roll on the setup CBCT the required corrections on the verification
CBCT vary widely. There is a moderate correlation between the magnitude of pitch
and the longitudinal correction and a strong correlation between the magnitude
of roll and the lateral correction. Very similar statistical data and
correlation coefficients show that the subgroups of breast cancer patients
correspond to those for the entire group and that the stability of breast
cancer patients is comparable to lung cancer patients.