Intrafraction prostate motion management in dose-escalated linac-based SBRT
PO-1716
Abstract
Intrafraction prostate motion management in dose-escalated linac-based SBRT
Authors: Denis Panizza1,2, Raffaella Lucchini3,2, Valeria Faccenda1,4, Martina Camilla Daniotti5, Paolo Caricato1,4, Sara Trivellato1, Stefano Arcangeli3,2, Elena De Ponti1,2
1ASST Monza, Medical Physics Department, Monza, Italy; 2University of Milan Bicocca, School of Medicine and Surgery, Milan, Italy; 3ASST Monza, Radiation Oncology Department, Monza, Italy; 4University of Milan, Department of Physics, Milan, Italy; 5University of Milan Bicocca, Department of Physics, Milan, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
This study reports the
pioneering clinical experience using an electromagnetic (EM) tracking device for
intrafraction prostate motion management during dose-escalated linac-based
SBRT.
Material and Methods
Thirteen patients with organ-confined prostate cancer underwent
dose-escalated SBRT using VMAT techniques with FFF beams on Linac platform. An integrated Foley catheter with a
transmitter in a dedicated lumen was used for intrafractional tracking. Patient
setup and target localization were achieved by CBCT matching. Treatment was
interrupted when the transmitter signals exceeded a 2 mm threshold in any of
the three spatial directions and, unless the offset was transient, treatment
target position was re-defined by repeating CBCT. A C++ code was implemented to
perform retrospective data analysis of the displacements along the three directional
axes. Moreover, adjusting setup and delivery phases duration, the developed
program enabled simulation of the displacements that would have occurred
without any organ motion management.
Results
Overall, intrafractional
tracking was successfully carried out in all the treatment sessions. In 31 out
of 56 monitored fractions (55%), no intervention was required to correct the
target position as a result of an excessive displacement. In 25 (45%) treatment
sessions, a correction was mandated, but only in 10 (18%) the beam delivery was
interrupted. Overall mean treatment time was 10.2 minutes [range 5.5 - 22.7]
with on average 3.5 minutes [range 2.5 - 7.3] for the gated beam delivery. The mean
value of the target average deviation during the whole session was -0.18 mm,
-0.01 mm, and -0.26 in lateral, longitudinal, and vertical
direction, respectively. The
prostate was found inside the 2 mm threshold from its initial position in 96%
of the treatment time, i.e. in 94% of the time during the setup phase and in
98% during the delivery phase (beam on + interruptions). Without any intrafraction
organ motion management, the overall mean treatment time and the mean delivery
time would have been 6.7 minutes [range 7.7 - 6.6] and 3.2 minutes [range 2.5 – 4.2],
respectively. The prostate would have been found outside the tolerance in 9% of
the session total time, i.e. in 4% of the time during the setup phase and in 16%
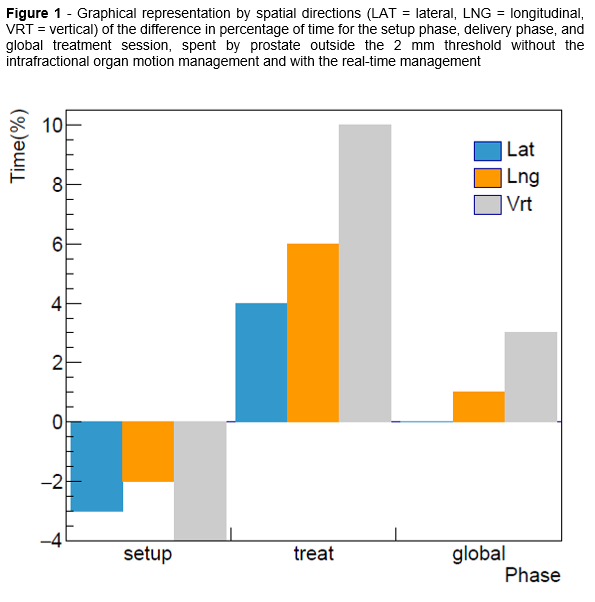
during the beam-on phase. The differences in the percentage of time spent by
the prostate outside the threshold in the three spatial directions between the
analysis without and with the organ motion management are shown in Figure 1.
Conclusion
Our findings show that
EM tracking is a reliable technique for real-time non-ionizing prostate
monitoring during dose-escalated SBRT, allowing to keep the target within 2 mm,
by interrupting the
beam delivery when the prostate was in an unsafe position. Without any intrafraction
motion management, both the setup and the delivery phases would have been
shorter, but significant displacements would have occurred leading to potential
target missing and overdose to organs at risk.