Dosimetric effect of uncorrected rotational errors during prostate SBRT Cyberknife treatments.
PO-1704
Abstract
Dosimetric effect of uncorrected rotational errors during prostate SBRT Cyberknife treatments.
Authors: David Sevillano1, Juan David García-Fuentes2, Asunción Hervás3, Carmen Vallejo3, Fernando López-Campos3, Rafael Colmenares4, Rafael Morís4, Belén Capuz4, Miguel Cámara4, Pedro Retorta4, Pablo Galiano4, Sandra Williamson4, María José Béjar4, Daniel Prieto4, Feliciano García-Vicente4
1H. U. Ramón y Cajal. IRYCIS, Medical Physics, Madrid, Spain; 2H. U. Ramón y Cajal, IRYCIS, Medical Physics, Madrid, Spain; 3H. U. Ramón y Cajal, IRYCIS., Radiation Oncology, Madrid, Spain; 4H. U. Ramón y Cajal, IRYCIS., Medical Physics, Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
The
Cyberknife system does only allow to perform rotational corrections if the
prostate position is within certain tolerances (±5 degrees in pitch and ±3
degrees in yaw and ±2 degrees in roll). When it is not possible to setup the
patient correctly, the user faces the decision of whether it is better to treat
without rotational corrections or try to reposition or even replan that treatment.
To ease this decision, this work studies the dosimetric effect of not applying
rotational corrections in prostate SBRT treatments with Cyberknife.
Material and Methods
17 prostate
SBRT treatments with Cyberknife were studied. Treatment plans consist on
delivering 36.25 Gy to the prostate+1/3 of seminal vesicles (SV) with an
isotropic CTV-to-PTV margin of 5mm. For each plan, the dose delivered to the
patient in one fraction was assessed by applying different rotational
systematic errors to the dose matrices. Intrafractional variations of these
rotations were also applied based on data from our patient population.
For each
treatment, errors from -10 to 10 degrees in pitch and from -5 to 5 degrees in
both roll and yaw were tested. Thus, for
each of these pitch/roll/yaw combinations, the D98 on both prostate and SV CTVs
were obtained, while D1cc and Dmax of the urethra was also included in the
analysis.
The
mean values of the 17 treatments at each point were fitted to a second grade 3D
polynomial.
Results
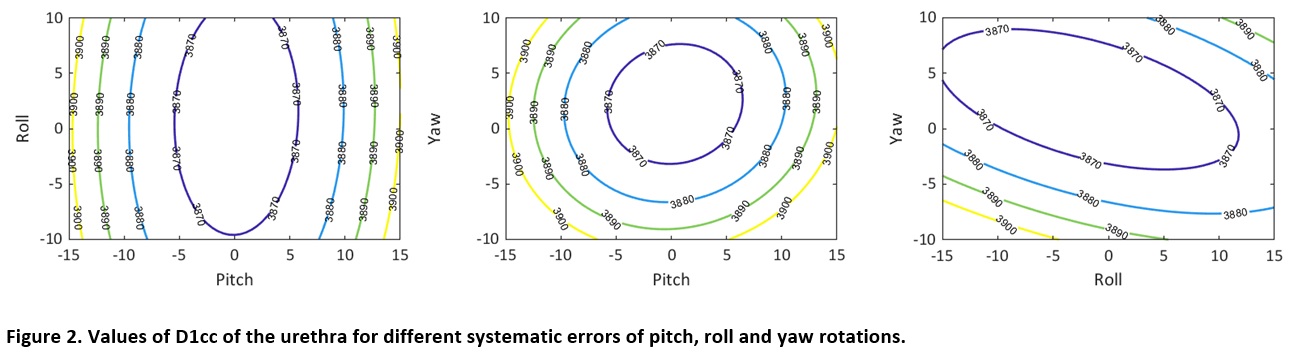
A 2D
representation of fitted values of prostate D98 and urethra D1cc at each plan
are shown in Figures 1 and 2. All fits yielded R2 values of 0.97, 0.97, 0.99
and 0.93 for D98 of prostate, D98 of SV, D1cc of urethra and Dmax of urethra
respectively.
Results
depended on the volume analysed, prostate D98 was above the prescription dose
of 36.26 Gy for all the rotations analysed, with dose being almost independent
of roll rotation. In the case of SV D98, pitch and yaw rotations of ±5 degrees
implied D98 less than 36.25 Gy but it was still over 34.4 Gy (90% of
prescription dose) for rotations within ±7.5 degrees. Again, SV D98 showed less
dependency with roll rotations for which ±10 degrees still assure a D98 of
36.25 Gy.
Regarding
the urethra, Dmax showed little variation with rotational errors, with
increases of up to 0.5 Gy for all rotations analysed, while D1cc of the urethra
could be higher than its constraint (38.78 Gy) for pitch and yaw rotations of
±7.5 degrees. Nevertheless, for pitch values of more than 10 degrees D1cc was
still below 39 Gy.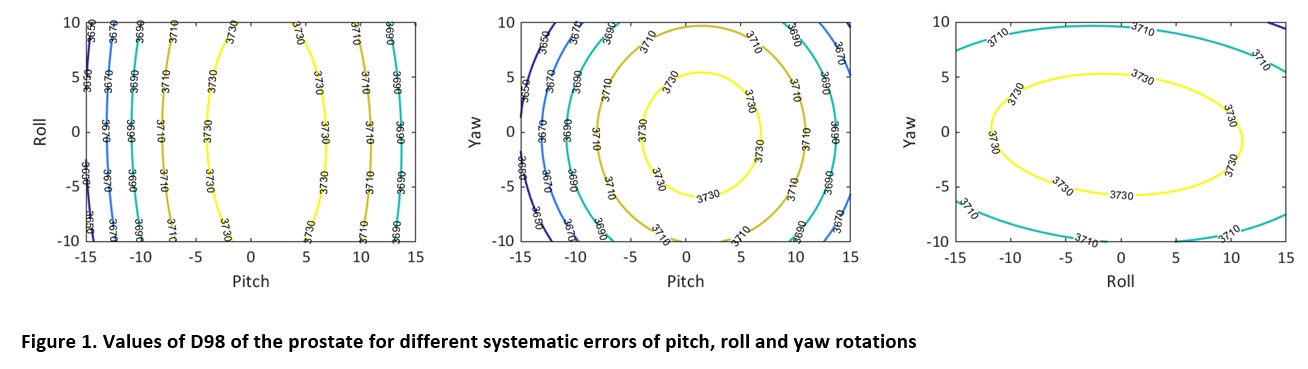
Conclusion
We have developed a useful tool to decide
whether it is safe to treat a prostate SBRT without rotational corrections for
a given fraction with Cyberknife. Nevertheless, if large errors appear systematically
for more than one fraction, an investigation of the reasons should be performed
and replanning should be considered.