Comparison of intra-fraction motion when using two distinct systems to perform DIBH in liver SBRT.
Alejandro Prado Barragán,
Spain
PO-1696
Abstract
Comparison of intra-fraction motion when using two distinct systems to perform DIBH in liver SBRT.
Authors: Alejandro Prado Barragán1, Daniel Zucca1, M. Ángel De la Casa1, Paz García2, Juan García2, Leyre Alonso1, Jaime Martí1, Ovidio Hernando3, Pedro Fernández-Letón4, Carmen Rubio4
1Hospital Universitario HM Sanchinarro. HM Hospitales, Medical Physics and Radiation Protection, Madrid, Spain; 2Hospital Universitario HM Puerta del Sur. HM Hospitales, Medical Physics and Radiation Protection, Madrid, Spain; 3Hospital Universitario HM Puerta del Sur. HM Hospitales, Radiation Oncology, Madrid, Spain; 4Hospital Universitario HM Sanchinarro. HM Hospitales, Medical Physics and Radiation Protection , Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
In
this work the intra-fraction (IF) motion was estimated through intra-fraction CBCT
(Elekta Medical) when DIBH was performed using Catalyst (CRad) or Active
Breathing Coordinator (Elekta Medical) in liver SBRT treatments.
Material and Methods
160
patients with liver metastases were considered. In 55 of them Catalyst was
utilized and for the other 105 ABC was employed. A total of 232 (479) IF CBCTs
were recorded for Catalyst (ABC). For every treatment session an IF CBCT was
synchronized with the first treatment arc. The full treatment was composed of
two arcs. The patient position was corrected before the second arc was
imparted. Using these corrections the IF motion for each patient and treatment
session was estimated.
Median values
and standard deviations were computed for each spatial component (SI, LR and
AP). Furthermore, the IF offset percentage lower than 5mm (O<5) and
the IF offset percentage greater than 8mm (O>8) were also
calculated. Moreover, systematic and random errors were obtained for each DIBH
systems employed. To elucidate whether there were significant differences in the
IF offset distribution widths between Catalyst and ABC IF motion data a
Fisher-Snedecor F test was performed with a 0.05 significance level.
Results
Table 1 shows medians, standard deviations and
systematic and random errors computed for SI, LR and AP. O<5 and
O>8 values were recorded in table 2. Both tables were arranged by
spatial component and DIBH system used. Distribution widths were statistically distinct, as p-values computed
through Fisher F-test were much lower than 0.001. Systematic and random errors
were higher in Catalyst treatments for all spatial components. For both DIBH
systems systematic and random errors were higher for SI direction. At least 81%
(90%) of the IF offsets were lower than 5mm and no more than 11% (4%) were
higher than 8mm in Catalyst (ABC) treatments. Lower O<5
and higher O>8 values were found for SI in both DIBH systems.
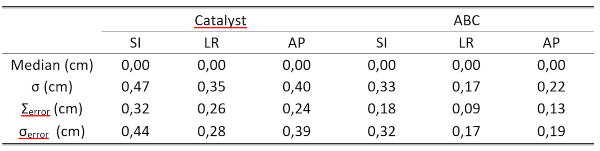
Table 1:
Medians, standard deviations and systematic (Σerror)
and random (σerror)
errors arranged by DIBH system and spatial component.

Table 2:
Percentage of IF offsets greater than 8mm (O>8mm)
and lower than 5mm (O<5mm) arranged by DIBH system and spatial component.
Conclusion
DIBH
reduces IF motion in liver SBRT but does not eliminate it completely, as some
residual motion is still present due to the imperfectness of breath-hold and
internal liver motion. Although
both systems are perfectly suitable to perform DIBH in liver SBRT, ABC is more
precise than Catalyst. These differences might be associated with the distinct
behavior of the respiratory cycle in the gated area. When utilizing ABC the air
flux is stopped and a completely flat respiratory pattern is obtained. However,
Catalyst forces the patient to hold its breath and to maintain the cycle inside
a gating window. Inside that window the respiratory cycle moves and so does the
patient. Further investigation should be perform to unravel IF liver motion
during SBRT treatments.