Potential NTCP reductions for high-risk prostate cancer patients by MR-guided adaptive radiotherapy
Rasmus Lübeck Christiansen,
Denmark
PO-1689
Abstract
Potential NTCP reductions for high-risk prostate cancer patients by MR-guided adaptive radiotherapy
Authors: Rasmus Lübeck Christiansen1,2, Lars Dysager3, Christian Rønn Hansen1,2, Tine Schytte3,2, Anders Smedegaard Bertelsen1, Henrik Robenhagen Jensen1, Faisal Mahmood1,2, Christina Junker Nyborg3, Steinbjørn Hansen3, Søren Nielsen Agergaard1, Olfred Hansen3,2, Carsten Brink1,2, Uffe Bernchou1,2
1Odense University Hospital, Laboratory of Radiation Physics, Odense, Denmark; 2University of Southern Denmark, Department of Clinical Research, Odense, Denmark; 3Odense University Hospital, Department of Oncology, Odense, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Daily,
MR-guided online adapted radiotherapy (MRgART) facilitates reduced PTV margins
in pelvic RT. This study investigates the potential benefit from MRgART in
terms of normal tissue complication probability (NTCP) in comparison to
standard CBCT linac treatment for high-risk prostate cancer patients.
Material and Methods
Twenty patients treated
for high-risk prostate cancer with 78 Gy to the prostate and proximal seminal
vesicles (CTV1) and 56 Gy to elective pelvic lymph nodes (CTV2) were included.
MR scans were acquired at simulation (pMR) and at the 10th, 20th
and 30th fraction (+/- 2) on a diagnostic scanner to simulate the
daily scans on a high field MR-linac (MRL). MRgART workflows were simulated in
offline Monaco 5.40 (Elekta AB, Stockholm, Sweden) with an MRL reference plan
on the planning MR with nine beams and up to 80 segments. An independent study
had previously shown that the appropriate PTV margins for MRgART were 5 mm
(AP), 4 mm (SI) and 3 mm (RL) for CTV1 and 2 mm for CTV2. A reference plan created
on the pMR was adapted to each of the three session scans, including contour
deformations, and the adapted plan doses were warped onto the pMR.
Standard plans were generated as single arc VMAT
plans with the aid of AutoPlan in Pinnacle 16 (Philips Medical Systems,
Madison, WI, USA). Our department standard PTV margins were applied as a uniform
7 mm addition to CTV1 and 7 mm (AP), 12 mm (SI) and 5 mm (RL) to CTV2, to
account for CBCT match on fiducials in the prostate. The standard RT plan was
rigidly registered to each adaptation MR before it was warped to the planning
MR for dose accumulation. Doses to organs at risk were compared by DVH analysis
and potential clinical effects were assessed via NTCP models from the literature.
Results
MRgART yielded
statistically significant lower doses for the bladder wall, rectum and
peritoneal cavity, compared to the standard RT, as exemplified in Figure 1.
Mean population accumulated doses were as good or better for all investigated organs
at risk (OAR) when planned for MRgART compared to standard RT. These reductions
in dose to the OAR translated into reduced median risks of hematuria (ΔNTCP 0.5%), urine incontinence (ΔNTCP 2.8%),
urine voiding pain (ΔNTCP 2.8%) and acute
gastrointestinal toxicity (ΔNTCP 17.4%), as illustrated in
Figure 2.
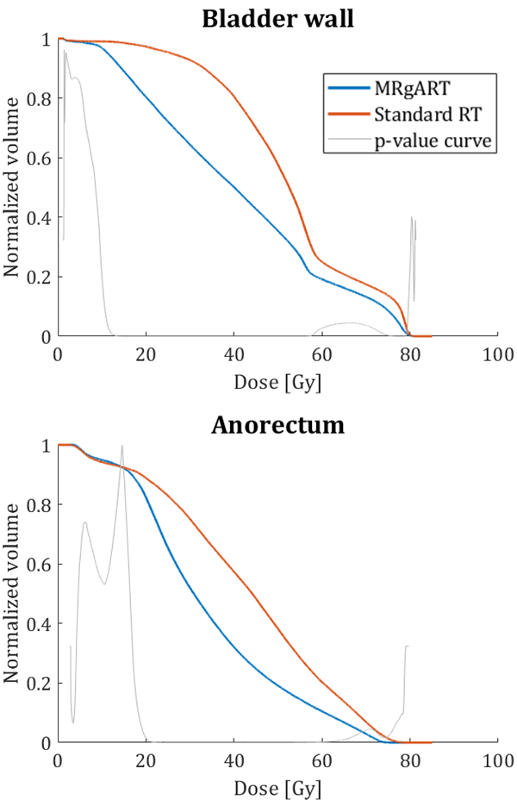
Figure 1. Population mean DVH from MRgART and standard RT for the
bladder wall and rectum. The p-value curve is a means to illustrate the dose
levels of statistical significant differences.
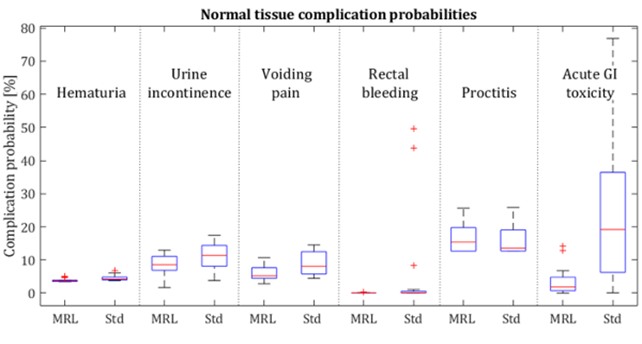
Figure 2. Boxplots showing the distribution of the
patients’ NTCP for investigated clinical endpoints from MRgART (MRL) and
standard RT plans (Std). Data points exceeding 1.5 times the interquartile
range are considered outliers and marked with a red +.
Conclusion
Online
adapted radiotherapy may reduce the dose to OAR in high-risk prostate cancer
patients, due to reduced PTV margins. This potentially translates to
significant and clinically relevant reductions in the risks of acute and late
adverse effects.