Prediction of heart and lung dose in breast cancer radiotherapy
Karina Lindberg Gottlieb,
Denmark
PO-1670
Abstract
Prediction of heart and lung dose in breast cancer radiotherapy
Authors: Karina Lindberg Gottlieb1, Martin Kjellgren1, Mette Holck Nielsen2, Kenni Højsgaard Engstrøm1, Ebbe Laugaard Lorenzen1
1Laboratory of Radiation Physics, Department of Oncology, Odense University Hospital, Odense, Denmark; 2Department of Oncology, Odense University Hospital, Odense, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
PlanIQTM (Sun
Nuclear) software provides a tool that uses target and organ at risk (OAR)
geometry to indicate the difficulty of achieving different doses for organ
dose-volume histograms. We investigate whether this tool can be used as a priori
estimation of the complexity of the plan. Is it possible to fulfill both goals
for covering the target while sparing the OAR or is it necessary to compromise?
This would be helpful upfront for the planner and oncologist to decide what to prioritize.
Material and Methods
108
breast cancer patients treated
with postoperative radiotherapy at Odense
University Hospital during 2020 were planned in Pinnacle3 (version 16.2.1)
and PlanIQ (version 2.2). The cohort of patients included both patients with
lumpectomy, mastectomy, and with and without lymph node involvement. A plan was
made in Pinnacle where all goals for the target (using DBCG
consensus guidelines) were fulfilled while sparing
the OAR as much as possible. Plan setup was a tangential field-in-field method.
All plans were sent to PlanIQ including the target and the OAR goals and PlanIQ
estimated the feasibility of fulfilling the OAR criteria while still fulfilling
the target criteria. 54 of the patients were randomly selected and used as training set in
order to fit a linear model relating PlanIQ doses (“predicted”) to Pinnacle
doses (“actual”). The remaining 54 patients were used as a test set for
validation of the fitted models.
Results
The linear
model fitted on the training data was:
μHeartDose=1.270‧μPlanIQ+0.577 and μLungDose=2.764‧μPlanIQ+0.166
μPlanIQ being the predicted dose from PlanIQ and μHeartDoseand μLungDose the mean heart and lung dose from Pinnacle
dose plans for optimal target coverage. The result of applying a linear model
to the training set is shown in Figure 1. a) and b). These plots show a
scatterplot of the actual dose versus the predicted dose for the mean heart dose
and mean ipsilateral lung dose respectively. Plot c) and d) shows Bland-Altman
plots for the same OAR. A good correlation was observed with R-squared values
of 0.93 and 0.96 for heart and ipsilateral lung respectively. 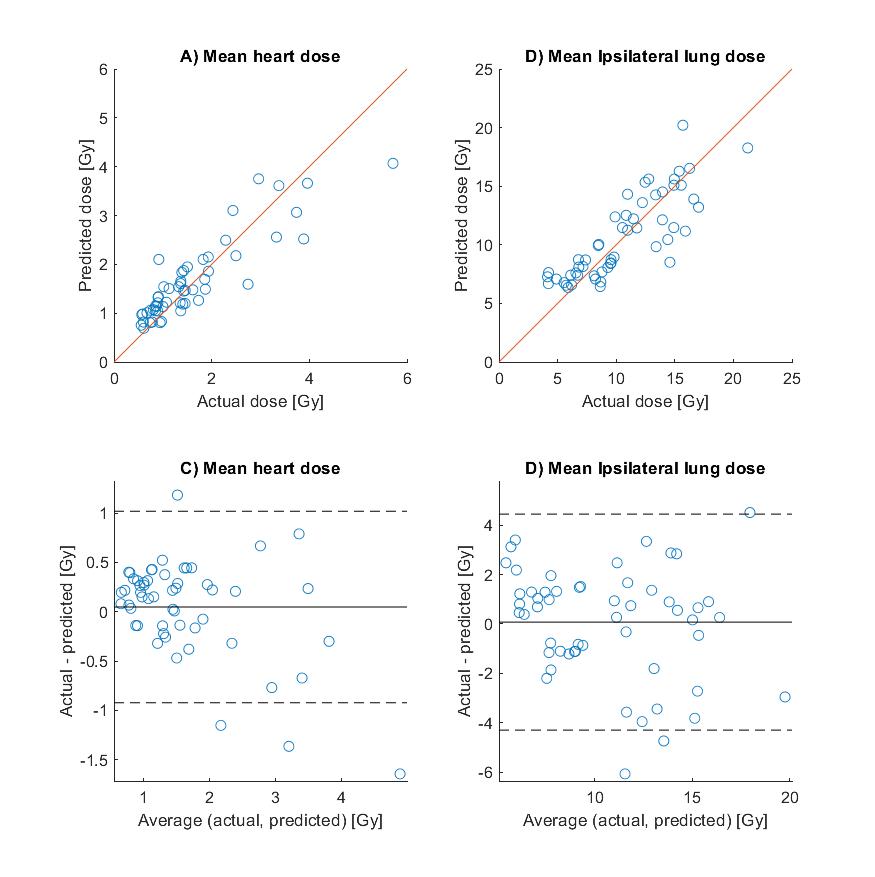
Figure 1:
a) and b) shows scatterplot
of the actual dose versus the predicted dose for the mean heart dose and mean
ipsilateral lung dose. c) and d) shows Bland-Altman plots for the same OAR,
where the dashed lines indicate the limits of agreements (95% confidence
interval).
Conclusion
PlanIQ shows to be useful to use as a quick prediction of
doses to heart and ipsilateral lung in breast cancer radiotherapy. This could allow for
early clinical decision-making on potential target compromises to keep doses to
organs at risk below specific levels. In addition, an early detection of
patients that could be candidates to proton therapy due to high dose to heart
or lung would be possible with PlanIQ.