Can auto-delineated lung lobe motion be a surrogate for tumour motion for Mid-V determination?
PO-1620
Abstract
Can auto-delineated lung lobe motion be a surrogate for tumour motion for Mid-V determination?
Authors: Evelien Bogaert1, Noémie Johnston1, Vincent Huybrechts1, Miet Vandemaele1, Frederik Vanhoutte1, Yolande Lievens1
1Ghent University Hospital, Radiation Oncology, Ghent, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
ESTRO-ACROP guidelines for radiotherapy of NSCLC recommend the use of a 4D breathing motion compensation strategy, e.g. respiration correlated 4DCT imaging for treatment planning (Rad.Oncol: 2017 Guckenberger and 2018 Nestle). Manual delineation of the tumour volume on multiple equally distributed time based phases of a 4DCT allows for Mid-Ventilation phase determination but is highly time consuming. Our goal was to investigate whether the motion of the centroid of an auto-delineated lung lobe, using a commercial software, can be a surrogate for tumour motion to determine Mid-V.
Material and Methods
For 30 patients, ten time-based phases following 4DCT imaging on a Siemens Go.Open Pro scanner equipped with Varian RGSC system were reconstructed. A manual delineation of the primary tumour bulk on all phases was done by a physician. The DirectORGANS algorithm (®Siemens Healthineers) generated the delineation of the five lobes on all phases. A global scoring (5 point scale) was performed, evaluating the following: anatomical correctness; appearance of holes or of wobbly edges; extension into soft tissue, shrinkage into lung tissue and consistency of the delineation over all phases.
The 10 bin Mid-V phase selection was performed using both tumour centroid and lobe centroid motion (TCM, LoCM). The lobe incorporating the tumour or adjacent to mediastinal tumours, was selected as the lobe of interest. The vector length difference of the distance to Mid-Position of the TCM compared to the LoCM was determined.
Results
Analysis was based on separate autodelineation per phase, due to unsatisfactory results of contour propagation by deformation with volumes preservation. This more laborious process resulted in an average quality score of 4.4. For one patient with lobectomy of the left upper lobe, the left sided autodelineation was unacceptable.
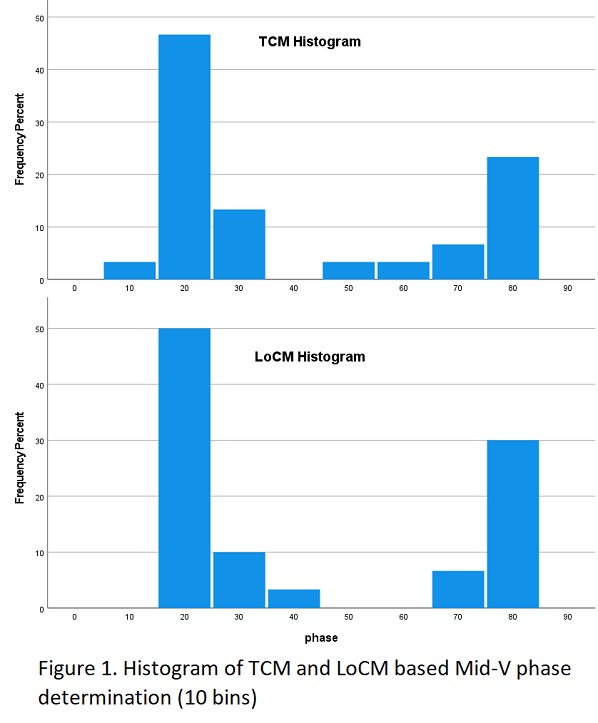
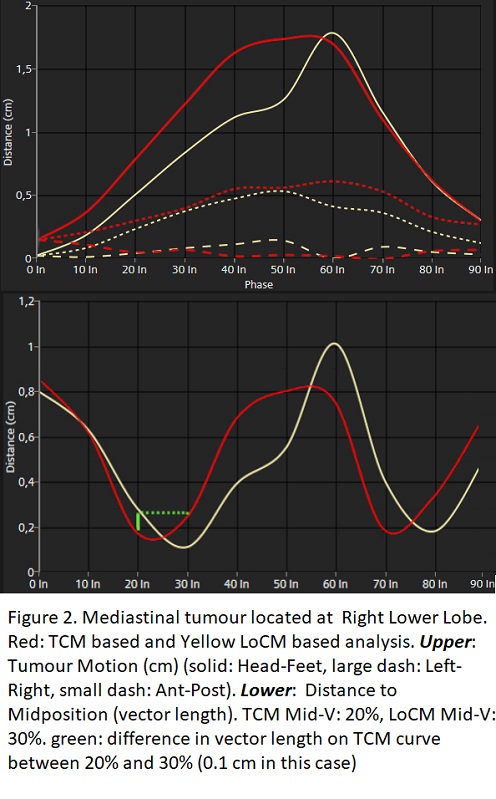
Histograms show that 20% phase-selection as Mid-V (during exhale) is predominant (frequency 46.7%), followed by 80%, 30% and 70% phases with an equivalent distribution in LoCM and TCM (Figure 1). For 13/30 cases, TCM and LoCM methods determined the same Mid-V phase. In case the TCM and LoCM indicate a different phase, the estimated error in terms of mean vector length difference is 0.03 cm (mean) with a 0.14 cm maximum. An example case can be found in Figure 2.
Different Mid-V phase selection can be attributed to non-respiratory movement of tumours connected to the chestwall, vertebra or mediastinum. Differences also appear when an oscillatory difference is seen between LoCM and TCM.
Conclusion
Overall, LoCM can be used as a surrogate for TCM based Mid-V determination, if:
- The autodelineation is qualitative and consistent over the phases
- Clinical evaluation is done on all phases, in three directions and on a movie loop
- Considering that in case the tumour shows small movement (attached to the chestwall, vertebra or mediastinum) the LoCM might be less representative
- When oscillatory motion is observed between LoCM and TCM, the tumour should be manually segmented