Low dose cone beam CT protocols for image-guided breast and pediatric treatments
PO-1605
Abstract
Low dose cone beam CT protocols for image-guided breast and pediatric treatments
Authors: Marianne Falk1, Robert Vorbau2, Mathias Westermark1, Markus Hulthén2, Giovanna Gagliardi1
1Karolinska University Hospital, Section of Radiotherapy and Engineering, Medical Radiation Physics and Nuclear Medicine, Stockholm, Sweden; 2Karolinska University Hospital, Section for X-ray physics, Medical Radiation Physics and Nuclear Medicine, Stockholm, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
Planar kV-imaging is often preferred over cone beam CT (CBCT) for breast and pediatric treatments, as it gives less imaging dose. These patient groups could benefit from IGRT with CBCT to reduce the set-up uncertainties; furthermore, in the case of cranial lesions, this technique allow for 6D corrections with the treatment couch. This study was performed in order to investigate the CBCT doses of thorax and head protocols and to create low dose protocols for breast and cranial pediatric treatments.
Material and Methods
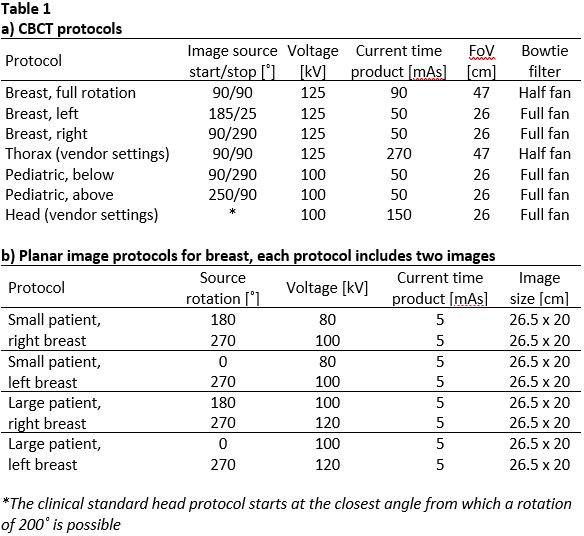
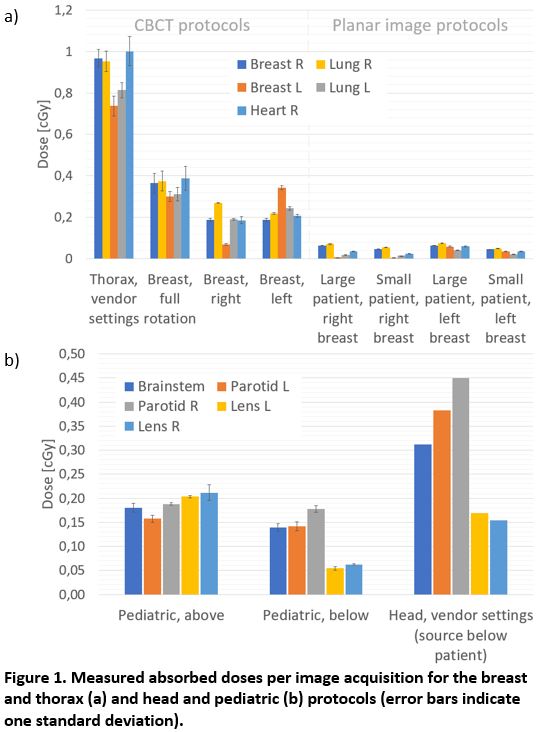
The low dose CBCT protocols were based on the vendor settings (Varian TrueBeam 2.7) and only different settings of the current-time product (mAs) and the irradiation angles were investigated. For the breast protocol, partial and full arc rotations were analysed with separate protocols for the right and left breast for the partial arc options and a smaller FoV (where the couch could not be centered for imaging if the breast and ribs were to be included). For the pediatric head protocol two scanning options were tested, with the imaging source sweeping below and above the patient respectively. Evaluation of the image quality and dose measurements were carried out using anthropomorphic phantoms with metal‐oxide‐semiconductor field‐effect transistor (MOSFET) detectors (Best Medical Canada) fitted into cavities in the lungs, breast and heart for the breast protocol measurements and in the brainstem, parotids and lenses for the pediatric head protocol measurements. For the tests of the pediatric protocols, a phantom similar in size to a one year old child were used. The MOSFET detectors were cross calibrated using an Exradin A2 ion chamber (Standard imaging). Measurements were also made for the planar imaging protocols used for breast patients in our clinic for comparison.
Results
The technical settings of the protocols are shown in table 1 and the measured results in figure 1. The effect on the image quality when the mAs was reduced to the lowest selectable setting was minimal and deemed acceptable for all cases. Since the couch could not be centered for the partial arc breast protocols, these protocols could not be used due to collision for a large portion of patients in our clinic (an adjustment of our standards for the treatment isocenter position could potentially solve this).
Conclusion
In our clinic, the breast protocol with full rotation is used for breast cancer patients as the increase of imaging dose compared to planar imaging was found to be acceptable. The reduced dose using a partial arc could not motivate adaptation of our standards for the isocenter position. For pediatric treatments, CBCT is only used when it is motivated, for example when 6D corrections of the couch is needed or the target is close to an organ at risk. In these cases, the protocol with reduced mAs and the imaging source sweeping below the patient is used as this gives the lowest doses to organs at risk.