Dose response of cuvette-sized versus bulk silicone-based radiochromic dosimeters
Morten Bjørn Jensen,
Denmark
PO-1538
Abstract
Dose response of cuvette-sized versus bulk silicone-based radiochromic dosimeters
Authors: Morten Bjørn Jensen1, Peter Balling2, Jørgen Breede Baltzer Petersen3, Simon J Doran4, Ludvig Paul Muren1
1Aarhus University Hospital, Danish Centre for Particle Therapy, Aarhus, Denmark; 2Aarhus University, Department of Physics and Astronomy, Aarhus, Denmark; 3Aarhus University Hospital, Department of Medical Physics, Aarhus, Denmark; 4The Institute of Cancer Research, Cancer Research UK Cancer Imaging Centre, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Silicone-based radiochromic
dosimeters allow for 3D dose verification with high spatial resolution. Key
dosimetric properties are often characterized using cuvette-sized dosimeters,
since 3D experiments are time consuming and costly. However, dosimetric
properties for larger samples must also be validated. The aim of this study was
therefore to assess the dose response obtained from cuvette-sized dosimeters
readout using a spectrophotometer versus larger cylindrical dosimeters readout
using an optical 3D CT scanner.
Material and Methods
Dosimeters were fabricated
from silicone elastomer, curing agent, chloroform and leucomalachite green from
a single batch and divided into two groups 1) 25 cuvettes (1 cm x 1 cm x 4.5
cm) and 2) 5 cylindrical dosimeters (height = 5 cm, diameter = 5 cm). Cuvettes
were placed between a 4.5 cm solid water (SW) build-up slab and a 5 cm SW
backscatter slab and irradiated to doses of 2, 5, 10, 15 and 20 Gy in a single
fraction with a beam quality of 6 MV and dose rate of 8.0 Gy/min. Five cuvettes
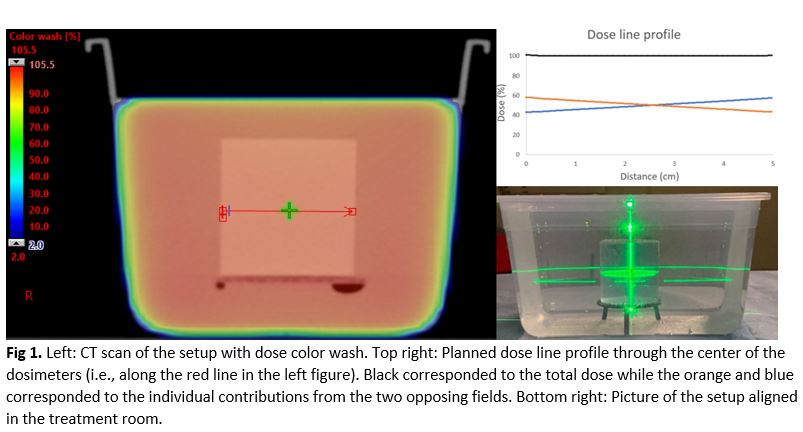
were irradiated simultaneously per dose level. The cylindrical dosimeters were
immersed in a water tank (Figure 1) and irradiated with two opposing 10 cm x 10
cm fields to obtain a uniform dose distribution throughout the dosimeters to doses
of 2, 4, 6, 8 and 10 Gy with 6 MV beam quality and a dose rate of 5.6 Gy/min.
The number of monitor units needed to deliver a given dose was calculated based
on a CT scan of the setup imported to the treatment planning system (Eclipse, Varian
Medical Systems). One cylindrical dosimeter was irradiated per dose level. The
dosimeters were readout prior to and after irradiation. Cuvettes were readout
using a spectrophotometer (Spectroquant Pharo 100) at 625 nm. Cylindrical
dosimeters were readout using a VistaTM 16 optical CT scanner (Modus
Medical Devices) at 635 nm and data reconstruction was performed with a
resolution of 1.0 mm x 1.0 mm x 1.0 mm, using an OSC-TV algorithm provided as
an integral part of the scanner. The dose response was given as the
irradiation-induced change in attenuation coefficient (averaged over a (5 x 5 x
5)-voxel region at the center of the cylindrical dosimeters) plotted against
dose.
Results
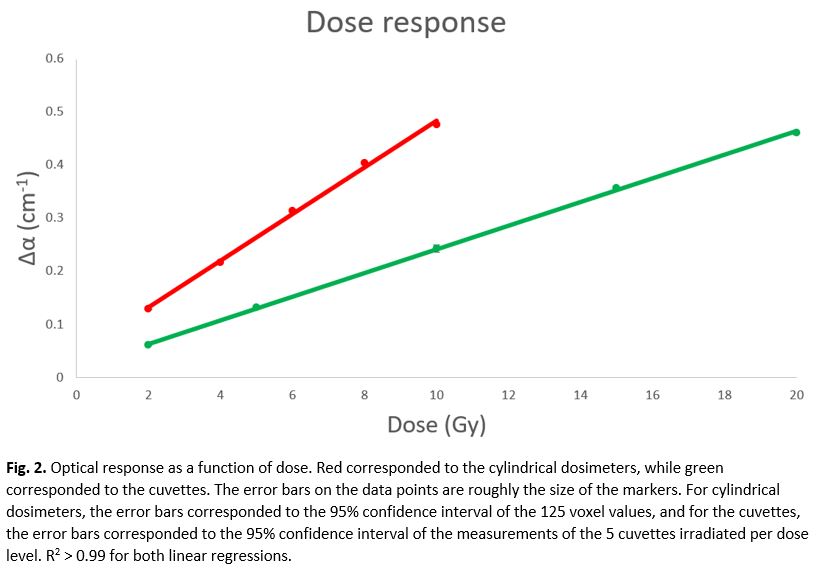
Linear dose responses were
found in the investigated dose ranges for both cuvettes and cylindrical
dosimeters (Figure 2). The dose response for the cuvettes was (0.022 ± 0.0003)
Gy-1cm-1 while it for the cylindrical dosimeters was (0.044
±
0.004) Gy-1cm-1.
Conclusion
The dose response reported for larger samples measured
using the optical CT scanner operating at 635 nm was greater than that for
cuvettes as reported by spectrophotometry at 625 nm. Further studies are needed
to determine whether the difference is related to variations in volume, shape,
readout modality or irradiation conditions. Both optical CT of large samples and spectrophotometry of
small samples provide high-quality relative measurements of absorbed dose. However,
careful calibration is needed to relate these two distinct types of experiments.