MR-guided adaptive versus CT-guided SBRT for prostate cancer: where is cost-benefit balance?
Alessandra Castelluccia,
Italy
PO-1401
Abstract
MR-guided adaptive versus CT-guided SBRT for prostate cancer: where is cost-benefit balance?
Authors: Alessandra Castelluccia1, Domenico Marchesano2, Gianmarco Grimaldi3, Ivan Annessi2, Federico Bianciardi2, Annamaria Di Palma2, Veronica Confaloni3, Federica Rea3, Barbara Tolu3, Maria Valentino2, Laura Verna2, Maria Rago2, Cristian Borrazzo2, Luca Capone3, Marica Masi2, Randa El Gawhary2, PierCarlo Gentile2,3
1San Pietro FBF, Radiantion Oncology, Rome, Italy; 2San Pietro FBF, Radiation Oncology, Rome, Italy; 3UPMC San Pietro FBF, Radiation Oncology, Rome, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
The purpose of this study is to compare different techniques of SBRT for localized prostate
cancer (PCa), stereotactic MR-guided adaptive RT (SMART) versus cone beam CT(CBCT)-guided
SBRT, in terms of toxicity and time costs.
Material and Methods
Patient with localized PCa (clinical stage T1-2bN0M0) underwent SBRT using CT-LINAC
system (True Beam STx, Varian) or MR-hybrid LINAC system (MRIdian, Viewray). SBRT was prescribed to a dose of 40
Gy (8 Gy/fr) and 36.75 Gy (7.25 Gy/fr) to prostate and PTV,
respectively, at 80% isodose, delivered on 5 days (3fr/week). An anisotropic 5mm-margin (3mm posterior) was created
around the prostate for the PTV. Treatment was delivered using two different
image guidance (IG) strategies. CT-guided SBRT strategy consisted of a
pre-treatment CBCT acquisition with implanted fiducial markers and images matching using the
ExacTrac® system. SMART consisted
of indentification of target and OARs on pre-treatment MR images, with on-line
calculation and delivery of a new plan for every fractions because of inter-fraction
variation of bladder and rectal filling. Then an intra-fraction motion
management strategy was applied,
consisting of a gating approach based on the real-time acquisition of a
sagittal cine MRI during the whole delivery time (temporal resolution: 8
frames/s). Mean time for each step of daily workflow was
recorded. Common Terminology Criteria for Adverse Events was used to score
gastrointestinal and genitourinary early toxicity during
3-month follow-up.
Results
Sixty patients (pts) treated with prostate SBRT were compared. Real-time adaptive MR-guided
RT strategy was used for 30 pts (50%) . Pre-treatment CBCT was performed in 150
treatments. Using CBCT-IG, grade 2 acute rectal toxicity occurred in 3 pts ; 1
pts with Grade 2 and 1 pts with grade 3
urinary toxicity were observed . No grade 2 and 3 toxicity was recorded for
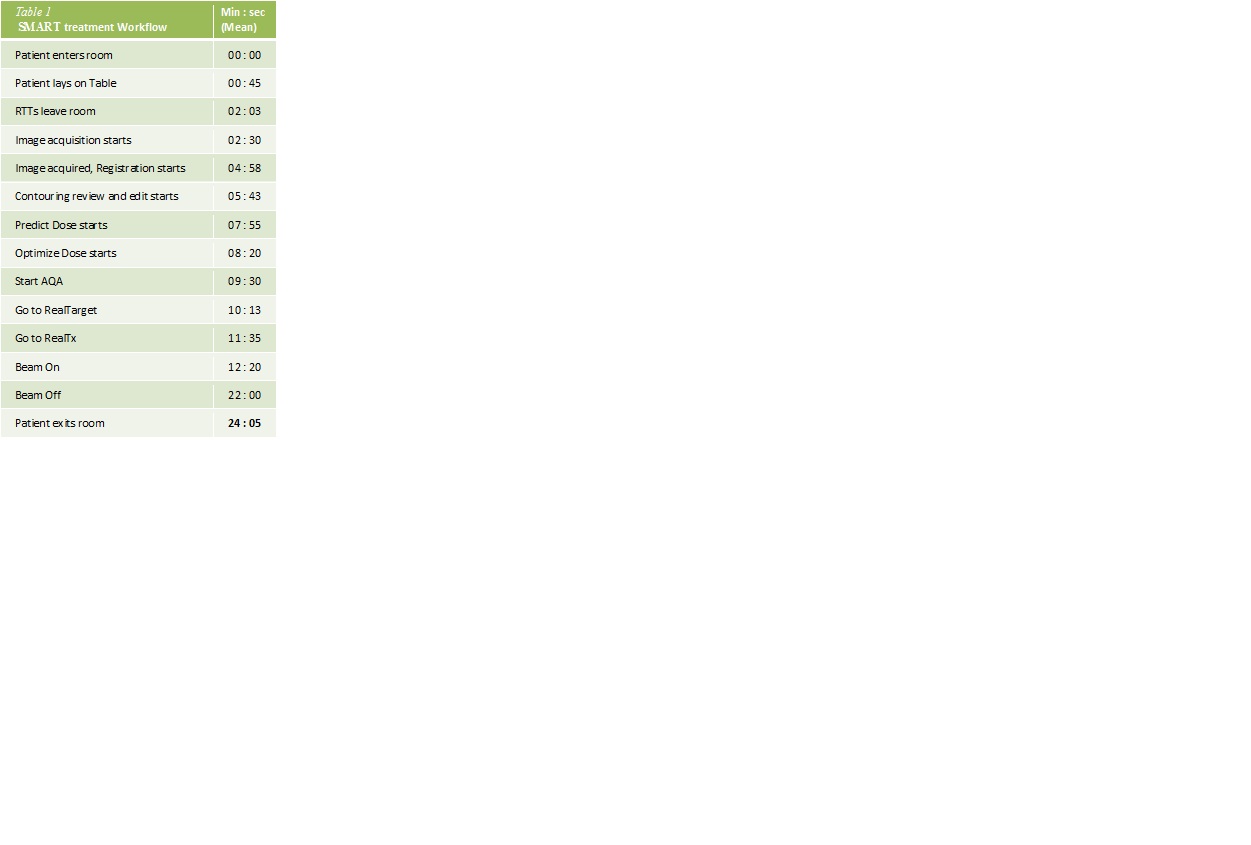
SMART treatments. Mean total daily treatment time was about 13 (range 11-17) and 24 (range 22-30) minutes for CT-guided SBRT
and SMART respectively. Treatment workflows are shown in table 1 and table 2.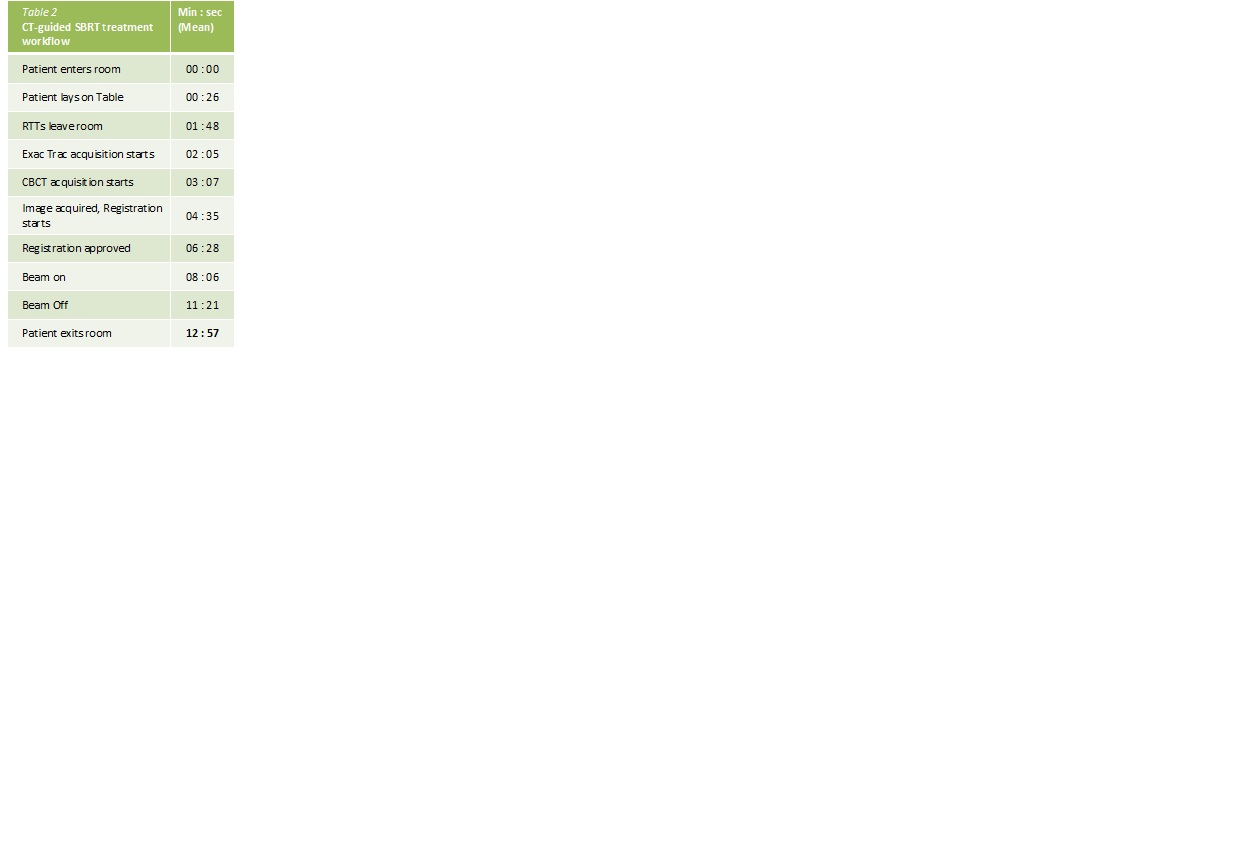
 .
.
Conclusion
SBRT for prostate cancer is a safe and effective
treatment. CT-guided SBRT involves acceptable
toxicity , however it needs additional equipment (ie. fiducials placement,
ExacTrac® system ) to assure interfraction organ-motion control and
delivery precision. SMART for prostate cancer confirms efficacy and can reduce toxicity:
on-line adaptive and real-tracking improve precision and safety , with a slight
difference in the time of daily treatment. Further studies to
evaluate the optimal balance between clinical advantages of SMART technologies
and additional cost in terms of time and complexity are needed.