HDR brachytherapy boost for cervical cancer: 4 fractionation scheme efficacy and toxicity analysis
PD-0560
Abstract
HDR brachytherapy boost for cervical cancer: 4 fractionation scheme efficacy and toxicity analysis
Authors: Maud Le Guyader1, Daniel Lam Cham Kee2, Jean-Michel Hannoun-Levi1, Mathieu Gautier3, Marie-Eve Chand Fouche1, Brice Thamphya4
1Centre Antoine Lacassagne, Department of radiation oncology, Nice, France; 2Pôle Santé République, Department of radiation oncology, Clermont-Ferrand, France; 3Centre Antoine Lacassagne, Department of radiation oncology, radiophysic, Nice, France; 4Centre Antoine Lacassagne, Department of statistics, Nice, France
Show Affiliations
Hide Affiliations
Purpose or Objective
Brachytherapy (BT) boost after radio-chemotherapy (RCT) is a standard of care in the management of locally advanced cervical cancer (LACC). As there is no consensus on high-dose-rate (HDR) BT fractionation schemes, our aim was to report the oncological outcome and toxicity profile of four different schemes using bi-fractionated HDR-BT.
Material and Methods
This was an observational, retrospective, single institution study for patients with LACC receiving a HDR-BT boost. The latter was performed with a single implant and single imaging done on day 1. The different fractionation schemes were: 7Gy+4x3.5Gy (group 1); 7Gy+4x4.5Gy (group 2); 3x7Gy (group 3) and 3x8Gy (group 4). Summation of EBRT and BT doses was performed by calculation of EQD2. As HDR-BT fractionation evolved (number of fractions, dose per fraction, overall BT time), EQD2(t) was calculated taking into account the time factor for D90CTVHR and D2cc of OARs for the different HDR-BT fractionation schemes. Local (LFS), nodal (NFS) and metastatic (MFS) recurrence-free survival as well as progression-free survival (PFS) and overall survival (OS) were analyzed. Acute (≤ 6 months) and late toxicities (> 6 months) were reported.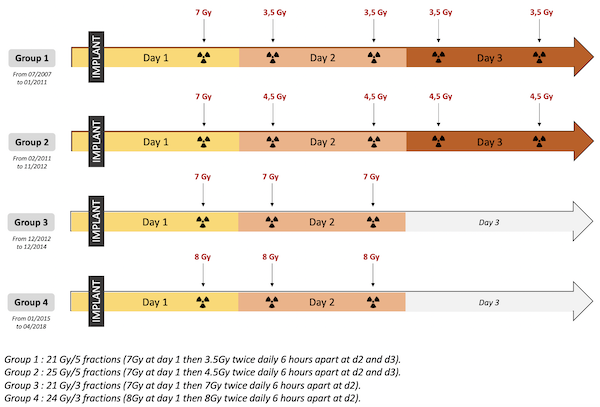
Results
From 2007 to 2018, 191 patients were included. Median follow-up was 57 months [45-132] and median EQD210D90CTVHR was 84, 82 and 90 Gy for groups 2, 3 and 4 respectively (dosimetric data missing for group 1). In group 4, EQD210D90CTVHR ≥85 Gy was achieved for 91% of patients versus 25% and 6% for groups 2 and 3 respectively. When calculating EQD2(t), we observed an increase of 8-9% for EQD210D90CTVHR and 5-10% for OARs EQD23D2cc. The 5-year LFS, NFS, MFS, PFS and OS were 85% [81-90], 83% [79-86], 70% [67-73], 61% [57-64] and 75% [69-78] respectively, with no significant difference between groups but a trend towards better local control in group 4 (5-year LFS : 90%). EQD210D90CTVHR<85Gy was a prognostic factor for local recurrence in univariate analysis (p=0.045). The rates of acute/late grade≥2 urinary, digestive and gynecological toxicities were 9%/15%, 3%/15% and 9%/25% respectively. A trend towards higher acute grade≥2 toxicities (p=0.061) and 2 late toxicities grade 4 were observed in group 4.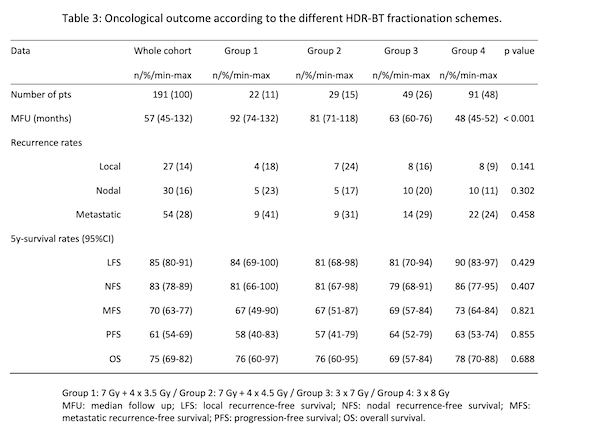
Conclusion
Bi-fractionated HDR-BT boost seems feasible with good oncological outcome especially after dose escalation but with slightly more toxicity.