To re-opt or not to re-opt: a study on the need for online plan adaptation for prostate cancer
Lisa Verweij,
The Netherlands
PD-0331
Abstract
To re-opt or not to re-opt: a study on the need for online plan adaptation for prostate cancer
Authors: Lisa Verweij1, Shyama U. Tetar1, Omar Bohoudi1, Berend J. Slotman1, Anna M.E. Bruynzeel1, Frank J. Lagerwaard1, Miguel A. Palacios1
1Amsterdam UMC, VUmc location, de Boelelaan 1117, 1081 HV, Department of Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Online adaptive MR-guided
radiotherapy (MRgRT) involves re-contouring and plan re-optimization prior to
each fraction to ensure adequate target coverage and maximal organ-at-risk
sparing. Additionally, in general adaptive MRgRT is delivered using only
minimal CTV to PTV safety margins. This online procedure is time-consuming and may
not always be needed, e.g. when the interfractional anatomical changes are
limited. In this study, we evaluated outcomes of target coverage and OAR doses
when plan re-optimization was not performed using CTV to PTV margins of 3mm and
5 mm, respectively.
Material and Methods
Ten patients with localized
prostate cancer previously treated with MRgRT in 36.25 Gy in 5 fractions were
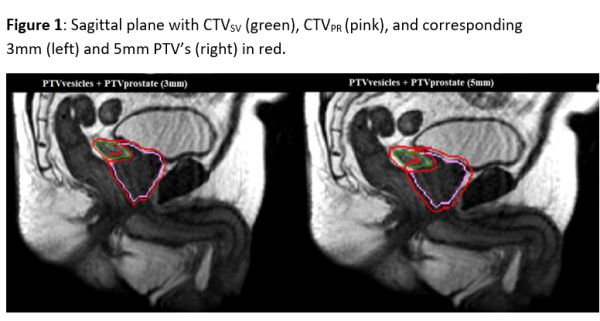
included in this study. The CTV was partitioned in a CTVPR
(prostate) and a CTVSV (seminal vesicles) by an experienced
radiation oncologist. This was performed for all six MR-scans available during MRgRT,
the simulation scan and high-resolution scans of fraction 1-5. All CTVs were
expanded with a 3 and 5 mm margin, respectively, generating a PTVPR_3mm,
PTVPR_5mm, PTVSV_3mm and PTVSV_5mm (Figure 1).
Baseline plans were generated for both the 3- and 5mm margin plans. After
alignment of the CTV, these baseline plans were recalculated for the anatomy of
the day on each pre-treatment MRI (non-reoptimized plans). Target dosimetry
(for both the 3- and 5mm plans) was evaluated by determining coverage of CTVPR
and CTVSV by the 95% isodose line for each of the 50 fractions. A CTV
coverage of V95% > 93% was considered as adequate. Doses to rectum and
bladder were determined to evaluate the effect of applying varying PTV margins to
relevant OARs.
Results
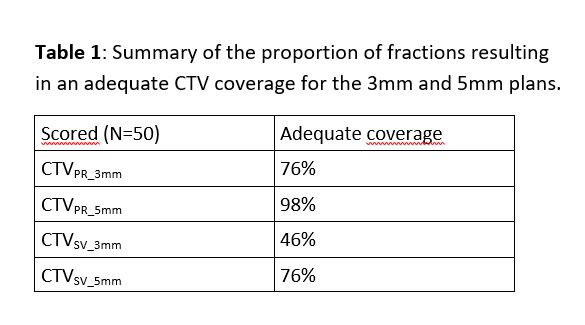
The 3mm CTV to PTV
margin plans had adequate coverage of the prostate and seminal vesicles in only
76% and 46%, respectively of all investigated 50 plans (Table 1). Increasing
the CTV to PTV margins to 5mm ensured adequate coverage of the prostate in all
but one fractions, however seminal vesicles coverage remained inadequate in 24%
of plans. The improved coverage using the 5mm margins came at a cost of OAR
doses. The bladder V100% and V90% increased on average 0.61cc
and 3.33cc, respectively (p<0.01).
Similarly, the rectum V100% and V90% increased 0.25cc and
1.77cc, respectively (p<0.01) in
comparison to the 3mm plans.
Conclusion
Without plan
re-optimization and use of a 3 mm PTV margin, coverage of the CTV’s of the
prostate and seminal vesicles was inadequate in about a quarter and half of the
fractions, respectively. Increasing the margins to 5mm corrected prostate
coverage at the expense of a higher OAR dose. Also with 5mm margins, coverage
of seminal vesicles was inadequate in approximately one quarter of plans. These
results underscore the need for routine online plan adaptation, particularly
when using 3mm margins. Use of implanted gold markers in the prostate for CTV
alignment on conventional linacs may be insufficient in intermediate- and
high-risk patients with SV involvement.