SBRT versus ENRT in oligometastatic gynaecologic tumors: techniques comparison.
Stefano Lorenzo Villa,
Italy
PD-0914
Abstract
SBRT versus ENRT in oligometastatic gynaecologic tumors: techniques comparison.
Authors: Stefano Lorenzo Villa1, Andrei Fodor1, Giuseppina Mandurino1, Flavia Zerbetto1, Chiara Lucrezia Deantoni1, Ariadna Sanchez Galvan2, Roberta Tummineri1, Simone Baroni1, Jessica Saddi1, Paola Mangili3, Roberta Castriconi3, Stefano Arcangeli4, Nadia Gisella Di Muzio1,5
1IRCCS San Raffaele Scientific Institute, Radiotherapy, Milan, Italy; 2IRCCS San Raffaele Scientific Institute, Radiotherapy, Milano, Italy; 3IRCCS San Raffaele Scientific Institute, Medical Physics, Milan, Italy; 4University of "Milano-Bicocca", Radiotherapy, Milan, Italy; 5“Vita-Salute San Raffaele” University, Radiotherapy, Milan, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
To compare
outcomes and toxicity of salvage extended nodal radiotherapy (ENRT) versus
Stereotactic body radiotherapy (SBRT) on lymph nodal (LN) relapse in oligometastatic
gynecological cancer patients (pts).
Material and Methods
From
03/2007 to 10/2021, 53 gynecological cancer patients with LN relapse after
previous radical therapies were treated with fluoro-deoxy-glucose positron
emission tomography/computed tomography (PET/CT) guided-salvage RT in our
Institution: 28 with ENRT+SiB on positive PET/TC LN (group 1) and 25 with SBRT
(group 2) on positive PET/TC LN. Primary histology was: ovarian in 20pts, endometrial
in 18pts, cervix in 11pts and others in 3pts, almost equally distributed in the
two groups. In group 1 two target were defined: the first one included the
lymph-nodal chain of interest (pelvic, para-aortic or mediastinal) as clinical
target volume (CTV1), adding a 7mm isometric margin to obtain the planning
target volume (PTV1). The PTV2 was obtained adding a 5mm isometric margin to GTV-PET.
In group 2 the PTV was obtained adding 3 mm isometric margin to GTV-PET. The
prescription dose was 50.4Gy/28 fractions (fr) to PTV1 and median dose of 61.01
(50.4-65.5)Gy to PTV2 in group 1, while in group 2 the median dose to PTV was 36
(30-45)Gy in 3-5 fr (6-12Gy/fr). The treatment was delivered with TomoTherapy® or
RapidArc® (Varian Medical Systems, Palo Alto, CA) in group 1 and
CyberKnife®(Accuray, Sunnyvale, CA) in group 2.
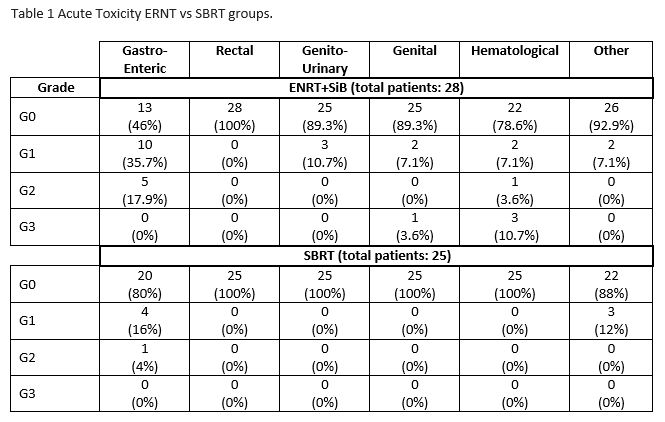
Results
Median
follow-up was 32.2 (3.4 – 142.4) and 14.67 (3.2-39.11) months for group 1 and 2,
respectively. Acute toxicity were almost negligible in SBRT and mild, in the
ENRT group, (see table 1). Loco-regional relapse was registered in 4/28 pts in group
1, while in group 2 relapse in lymph-nodal chain was registered in and 2/25 pts
and no recurrence occurred in the single lymph-node treated with SBRT. Systemic
progression was observed in 50% of pts in both group (53% vs 48%). Kaplan Meier
estimates of 12 months OS were 88% vs 93% (p=0,21), while 12-months DFS was 54
vs 58 % (p=0,99).
Conclusion
In oligometastatic
pts lymph-node PET-guided radiotherapy is feasible ensuring good (88.7%) local
control. Even considering the limitation due to the difference between the median
follow-up, of the two groups, the results seem similar in terms of DFS and OS.
ENRT+ SIB toxicity was acceptable but SBRT toxicity was lower. Longer follow-up
is necessary to confirm these results.