Robustness of spine SABR plans to delivery errors within machine tolerance: multicentre analysis
Mohammad Hussein,
United Kingdom
OC-0753
Abstract
Robustness of spine SABR plans to delivery errors within machine tolerance: multicentre analysis
Authors: Mohammad Hussein1, Joerg Lehmann2, Catharine Clark1,3
1National Physical Laboratory, Metrology for Medical Physics Centre, Teddington, United Kingdom; 2Calvary Mater Newcastle, Radiation Oncology, Newcastle, Australia; 3University College London Hospital, Medical Physics, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Spine SABR is characterised by delivery of
a highly localised dose to the PTV with sharp fall-off to spare surrounding
tissues, with a narrow trade-off between target coverage and sparing. Many
centres use conventional linacs run to machine tolerances specified for
standard treatments. The aim of this study was to investigate the robustness of
spine SABR treatment plans to simulated delivery errors that are within machine
tolerance in a multicentre setting.
Material and Methods
Fourteen centres participated in the study.
Each created a spine SABR plan following provided guidelines and sent it to the
study investigators. Custom Matlab software was used to introduce eight
different treatment delivery errors into individual copies of the DICOM plan
file, which were within machine tolerance. The same errors were introduced for each centre. Plans were then returned to the centres for dose calculation. Errors included
changes in collimator rotation, position of whole leaf banks of the MLC, and
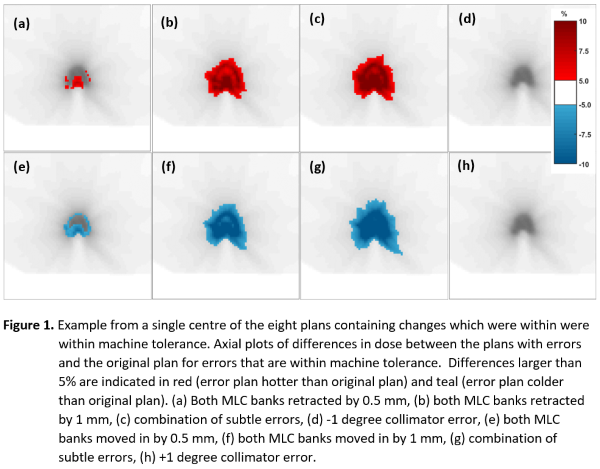
combinations of these together with changes in machine dose output. Description of the errors shown in Figure 1. The planning systems were
Eclipse, Pinnacle, Raystation, iPlan, Monaco and Oncentra MasterPlan. Linacs
were Elekta Synergy, Elekta Versa HD, Varian Clinac and Varian Truebeam. Centre
calculated dose distributions were resubmitted from which the near maximum
spinal cord dose (D0.03cc,SC) and dose to 90% of PTV (D90,PTV) were calculated centrally. To
assess individual impact of the error plans, the changes in
D0.03cc,SC and D90,PTV in the plan with the error versus
in the original plan were evaluated. Centres performed patient-specific QA
(PSQA) of each plan and reported a pass or fail according to their local
procedures.
Results
Figure 1 shows example axial plots of
differences in dose between the plans with errors and the original plan. Four
of the error plans caused a dose increase relative to the original plan, while
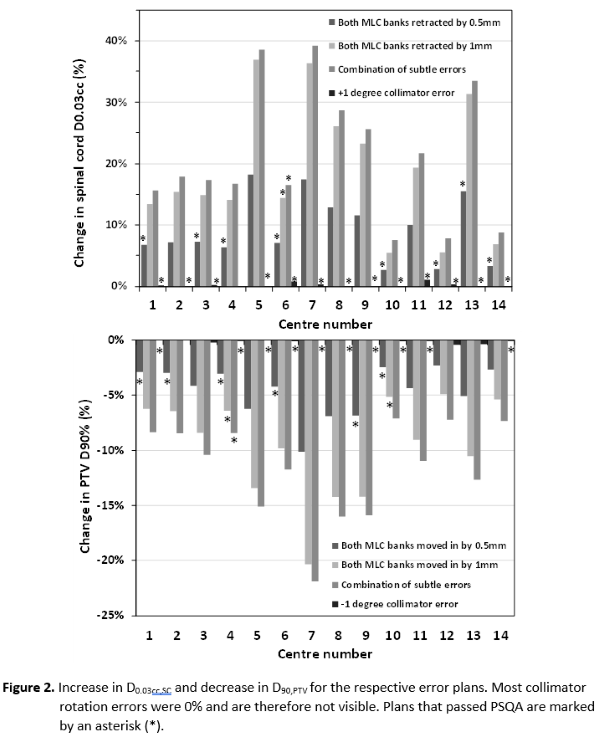
the remaining plans caused a dose reduction. Figure 2 shows the increase in D0.03cc,SC and decrease D90,PTV for the respective error plans. Plans that passed
PSQA are marked by an asterisk over each respective bar. A 1-degree collimator error in either direction did not cause any
significant change in any centre’s dose distribution. A 0.5mm retraction of
both MLC banks caused a >5% different D0.03cc,SC in 12 out of 14 centres. In
7 cases where the error caused a >5% difference in D0.03cc,SC and
in 4 cases where the error caused >5% reduction in D90,PTV, the
plans passed PSQA.
Conclusion
This study highlights that small errors,
some of which are well within machine tolerance specifications, can have
significant dosimetric impact on spine SABR plans. Furthermore, it was shown
that PSQA can miss some of these errors. The robustness of such plans to subtle
errors and PSQA tolerances should be carefully considered.