Knowledge-Based automatic plan optimization for whole breast Radiotherapy with Halcyon®
PD-0728
Abstract
Knowledge-Based automatic plan optimization for whole breast Radiotherapy with Halcyon®
Authors: Aldo Mazzilli1, Giovanna Benecchi1, Michele Maddalo1, Roberta Castriconi2, Claudio Fiorino2, Nunziata D'Abbiero3, Caterina Ghetti1
1University Hospital of Parma AOUP, Medical Physics, Parma, Italy; 2IRCCS San Raffaele Scientific Institute, Medical Physics, Milano, Italy; 3University Hospital of Parma AOUP, Radiotherapy, Parma, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
To adapt a Knowledge-Based (KB)-automatic planning approach for right-sided (R) tangential fields (TF) whole breast treatment using the volumetric technique ViTAT (Virtual Tangential Arc Therapy) with 6MV FFF (Free Flattening Filter) on Halcyon (Varian Inc.).
Material and Methods
An automatic KB-planning approach using ViTAT, that mimics TF, was previously validated and implemented. The KB-model was based on 100 TF plans delivered by the TrueBeam Linac and trained by the RapidPlan (RP) tool implemented in the Eclipse TPS (vs. 15.6, Varian).
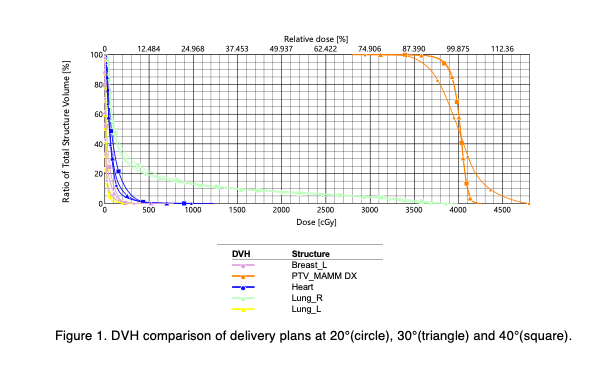
The clinical activation of the new Halcyon Linac, which uses only a 6MV FFF beam, brought out the need to adapt the model to this new equipment. 25 patients were selected and ViTAT plans were created on Halcyon, consisting of 4 arcs with start/stop angles consistent with the developed KB model (60°/220°); the arcs are completely blocked, except for the first and last 20° of rotation. Plan optimization was fully automated through the previously developed optimization template, based on the KB-model. As expected, the resulting Halcyon plans show an unacceptably inhomogeneous dose distribution, due to the FFF beam. To make the dose distribution homogeneous, compensating for the effect of the FFF beam, we tested the effect of increasing the beam delivery angles from 20° to 30° and 40°, keeping the start/stop angles of the arcs unchanged. Also in these cases, we used fully automated planning using the same optimization template. A comparison was made of the plans obtained in terms of OARs/PTVs dose-volume parameters. Wilcoxon-tests were performed to assess statistically significant differences (p<0.05).
Results
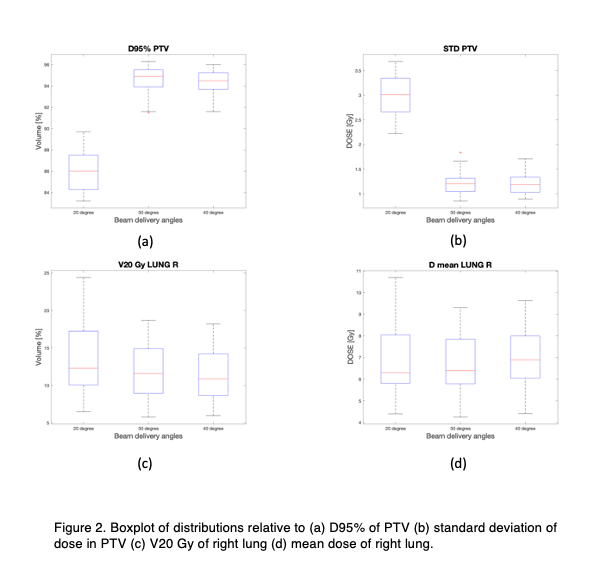
Plans obtained with beam delivery angles of 20° were all unacceptable in terms of PTV coverage (median D95%=86%), while the plans obtained by increasing the beam delivery angles to 30° and 40° were clinically acceptable (D95%=94.9% and 94.5% respectively). The homogeneity of the PTV dose distribution, through its standard deviation (STD), was significantly worse for the 20° plans compared to the 30° and 40° plans (p<0.05), while was not statistically significant between 30° and 40°. It is intriguing to note that, by increasing the angles of delivery, DVHs of the OARs do not undergo significant variations. Mean dose (Dm) and V20 of the right lung, were not significantly different (median V20<14%; Dm<7Gy). The heart (H) left breast (LB), and left lung (LL) showed low Dm (H<0.8Gy; LB<0.4Gy; LL<0.2Gy) with statistically significant differences only between 20° and 40°.
Conclusion
We proposed an approach to adapt the ViTAT technique using a 6MV FFF beam on Halcyon. The 20° beam delivery angle originally set for the ViTAT is not sufficient to achieve clinically acceptable coverage of the PTV. Increasing the delivery angle to 30°/40° resulted in optimal PTV coverage, maintaining similar sparing of the OARs. The clinical implementation of fully automatic plan optimization for R whole breast with Halcyon by this adapted ViTAT is ongoing.