CyberKnife vs protons: What is the best approach to reduce complications in posterior ocular tumors?
Emmanuelle Fleury,
The Netherlands
PD-0727
Abstract
CyberKnife vs protons: What is the best approach to reduce complications in posterior ocular tumors?
Authors: Emmanuelle Fleury1,3, Petra Trnková2, Caroline van Rij1, Nicole Naus4, Emine Kiliç4,5, Wilhelm den Toom1, Jean-Philippe Pignol6, Mischa Hoogeman1,3
1Erasmus Medical Center, Radiotherapy, Rotterdam, The Netherlands; 2Medical University of Vienna, Department of Radiation Oncology, Vienna, Austria; 3Holland Proton Therapy Center, Radiation Oncology, Delft, The Netherlands; 4Erasmus Medical Center, Department of Ophthalmology, Rotterdam, The Netherlands; 5Erasmus Medical Center, Department of Clinical Genetics, Rotterdam, The Netherlands; 6Dalhousie University, Department of Radiation Oncology, Halifax, Canada
Show Affiliations
Hide Affiliations
Purpose or Objective
Both fractionated stereotactic radiotherapy with CyberKnife
(CK) and ocular proton beam therapy with a dedicated ocular beamline have proven
to be successful eye-conserving treatments for uveal melanoma patients. Both
modalities have reported a high local tumor control in the literature, but comparative
data are lacking regarding the likelihood of post-therapy ocular complications
derived from imaging-based planning. This dosimetric study aims to evaluate and
compare the potential radiation-induced secondary complications assessed in clinical
CK plans vs. proton plans, which were simulated in line with the clinical
one-beam practice using a dedicated ocular beamline.
Material and Methods
Retrospective
CT-based treatment plans of 16 patients with critical posterior tumors in the
eye were used in this study. All tumors had T1 T2 staging and were abutting the
optic nerve within 3 mm. Patients were previously treated with a total CK dose
of 50 GyRBE in 5 fractions prescribed at the 80% isodose line (clinical plans).
Corresponding proton plans were simulated with a 60 GyRBE dose prescribed at
the 90% isodose line to be delivered in 4 fractions according to clinical
protocol. For the proton plans, individual gazing angles were selected to prioritize
the optic nerve and macula sparing. Dosimetric parameter values (D2%,
D20%, D25%, Dmean) were selected as predictors
of radiation-induced toxicity and were compared between both modalities. Patient-specific
spider maps were used to compare the dosimetric parameters and the risk and
severity of the main radiogenic side-effects with each treatment. Two-sided
Wilcoxon signed-rank tests were used to assess the statistical significance
(p-value<.05) of the dosimetric differences between modalities.
Results
Tumor coverage was reached for all patients with both
modalities: median Dmean=59.8 (CK) vs. 58.9 GyRBE (proton plans).
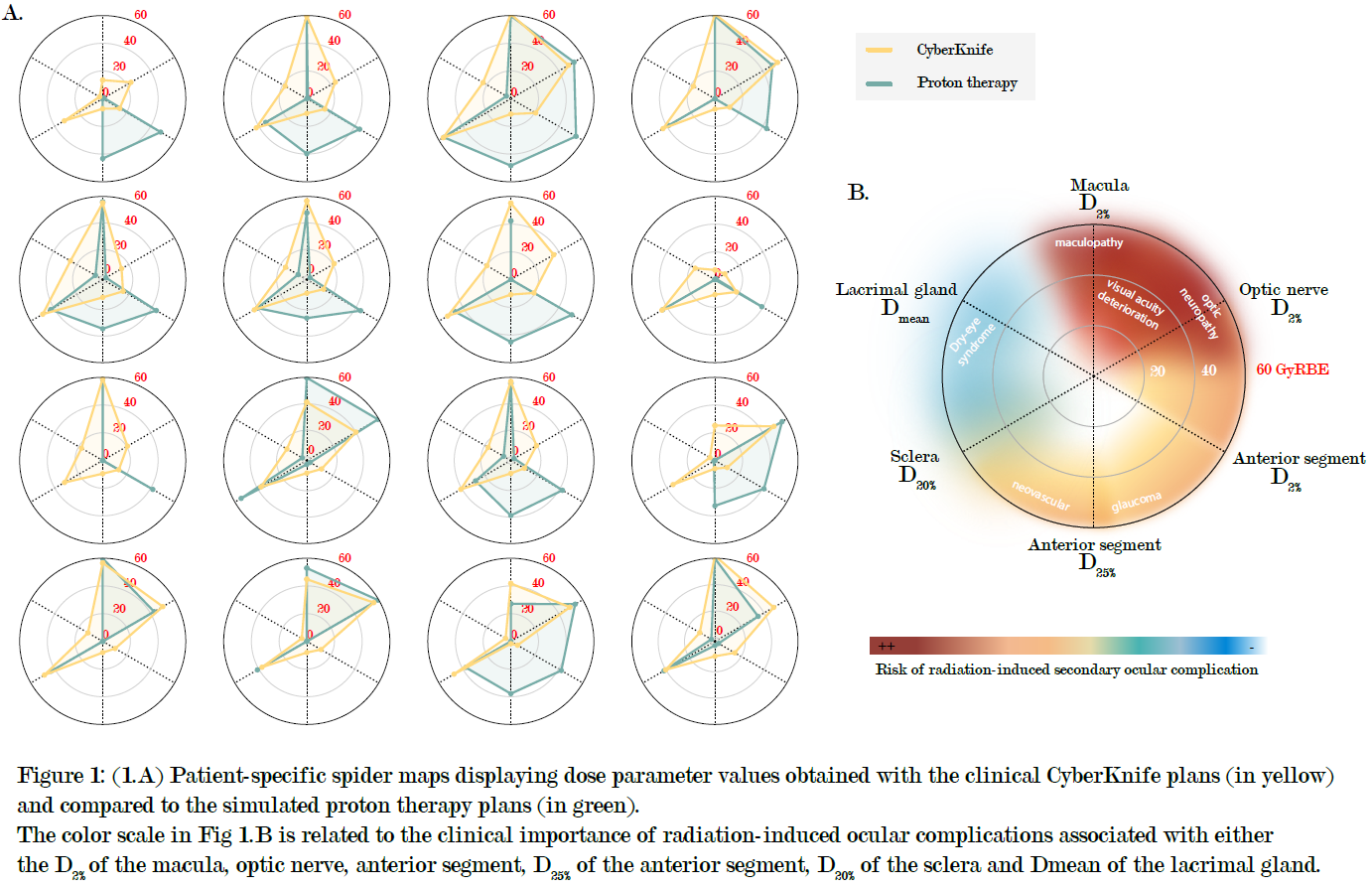
The spider maps are shown in Fig.1A, and the associated ocular risk and
severity in Fig.1B. In 11/16 patiens, the CK plans increased the D2% of
the optic nerve compared to the proton plans (median=38.0 vs. 17.9 GyRBE,
p-value=0.019, respectively), and the D2% of the lacrimal gland
(median 16.1 vs. 0.0 GyRBE, p-value<0.001, respectively). The same dose level
for the D2% of the macula and D20% of the sclera was
reported. Lastly, a decrease in both D2% (median=12.9 vs. 42.2 GyRBE,
p-value=0.002, respectively) and D25% (median=8.1 vs. 29.6 GyRBE,
p-value=0.038, respectively) of the anterior segment was obtained with CK
compared to protons.
Conclusion
Whereas proton
therapy has the potential to decrease the risk of optic neuropathy and dry-eye
syndrome compared to CK, radiation-induced complications occurring in the
anterior segment of the eye (ie neovascular glaucoma) are lower with CK. Radiation-induced
indicator tools as presented in this work could support the decision-making
process of choosing the most appropriate treatment for uveal melanoma patients.