Assessing the extent of treatment delivery errors among IROC H&N and lung phantoms
PD-0738
Abstract
Assessing the extent of treatment delivery errors among IROC H&N and lung phantoms
Authors: Sharbacha Edward1, Rebecca Howell1, Peter Balter1, Christine Peterson2, Julianne Pollard-Larkin1, Stephen Kry1
1MD Anderson Cancer Center, Radiation Physics, Houston, TX, USA; 2MD Anderson Cancer Center, Biostatistics, Houston, TX, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
The Imaging and Radiation Oncology Core (IROC) head and neck (H&N) and lung phantoms, used as an end-to-end test of an institution's radiotherapy treatment process, has an average failure rate of 14%. This work investigates whether delivery log files predict the observed dose deviations in these phantom irradiations.
Material and Methods
Delivery log files were collected for IROC lung and H&N phantoms irradiated by various institutions from January 2019 to present. We evaluated
these files in Mobius FX to determine the difference between the TPS-calculated
and machine-delivered doses (as a perturbation of the TPS). We evaluated
whether this perturbed dose more accurately predicted the actual delivered dose, measured by the thermoluminescent dosimeter (TLD). A total of 41 lung phantoms (82 TLDs) and 36 H&N
phantoms (216 TLDs) were evaluated. The maximum root-mean-square (RMS) errors in the MLCs, jaws,
collimators, and gantry angles during treatment delivery were also analyzed for
correlations with delivered dose.
Results
Compared to the average dose deviation (TPS vs TLD) of 2.4%
(max = 11.6%) for the H&N phantom, and 2.6% (max = 9.6%) for the lung
phantom, the dose perturbations predicted by log files were relatively small.
The delivery errors ranged between -0.73% to 1.20% for the H&N phantom.
Delivery played an even smaller role for the lung, which had a range of -0.75%
to 0.17%. Minimal correlation between dose deviation and delivery error was found:
r = .13 (p = .04) for H&N, r = .03 (p = .7) for lung.
Delivered dose was not strongly correlated with jaw, collimator,
or gantry angle maximum RMS errors (-0.2 < r < ± 0.2). MLC RMS error results for the two Varian
machine classes: Truebeam (including Edge) and the older Base model (iX, EX
& Trilogy), showed that the Truebeam machine MLCs performed better among
both phantoms. This difference, however, was not great enough to influence
phantom irradiation accuracy (Fig. 1).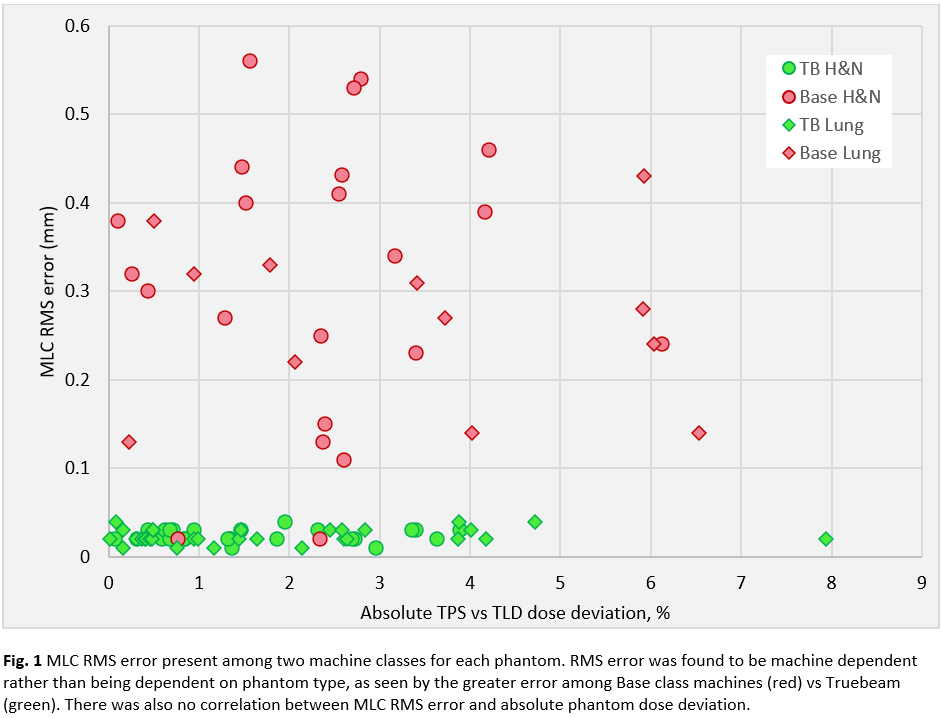
Conclusion
Analysis of IROC H&N and lung phantom delivery log files
showed minimal contributions to the total TLD dose deviations seen among these
phantoms. This indicates that few delivery errors are present, or that these
errors are not properly captured within the delivery log files. Future work will
investigate the ability of this delivery data to catch/identify irradiation
errors in IROC phantoms.