Changes in cortical blood flow >1 year after radiation for glioma using arterial spin labelling MRI
Michael Kosmin,
United Kingdom
PD-0245
Abstract
Changes in cortical blood flow >1 year after radiation for glioma using arterial spin labelling MRI
Authors: Michael Kosmin1, Meetakshi Gupta1, Magdalena Sokolska2, Björn Eiben3, Julia Markus4, Harpreet Hyare4
1University College London Hospitals NHS Foundation Trust, Radiotherapy, London, United Kingdom; 2University College London Hospitals NHS Foundation Trust, Medical Physics and Biomedical Engineering, London, United Kingdom; 3University College London, Radiotherapy Image Computing Group, London, United Kingdom; 4University College London Hospitals NHS Foundation Trust, Neuroradiology, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Radiotherapy (RT) plays a vital role in management of brain malignancies, but is associated with significant late effects including neurocognitive impairment and stroke. Quantifying long term changes in brain parenchyma could help in refining RT planning and monitoring for toxicities more effectively.
Arterial spin labelling (ASL) magnetic resonance imaging (MRI) uses the magnetisation of arterial blood water protons as an endogenous tracer, thus excluding the need for contrast injection. Early changes in cerebral blood flow (CBF) have been described after RT. We have developed a data framework that has enabled a retrospective study to determine whether CBF changes outside the treatment target are seen on ASL-MRI beyond one year after RT, and whether these correlate with delivered dose.
Material and Methods
Glioma patients who received high dose RT (54-60Gy) who had also undergone ASL-MRI 12-18 months after completion of RT at our centre were identified from our institutional databases and electronic medical records for inclusion.
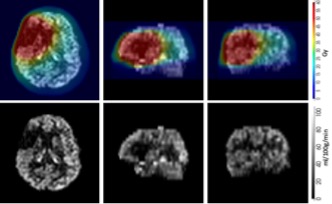
ASL was performed using pseudo-continuous labelling (pCASL) and 2D EPI readout on a 3T MRI (Achieva or Ingenia, Philips Medical Systems, Best, The Netherlands). Individual ASL volumes were first motion corrected using rigid registration (DTI-TK package) and quantified using simplified Buxton model. Cortex voxels were defined within CBF maps using a threshold (30-120ml/100g/min). RT dose data and planning CT images were exported from Eclipse (Varian Medical Systems, Palo Alto, USA), converted, and aligned to pre-contrast high resolution T1-weighted image (FSL package). Next, dose maps were down-sampled to CBF map resolution (Figure 1). Finally, RT dose was divided into six bins, and CBF data were normalised to the maximum value from the lowest dose bin and obtained for all subjects.
Results
Fifty four patients were identified as suitable for inclusion. Approximately 90 percent had pathologically confirmed high grade glioma (WHO Grade III/IV) and received RT doses of 59.4-60Gy in 1.8-2Gy daily fractions, with most of the remainder receiving 54Gy in 1.8Gy daily fractions for WHO Grade II tumours.
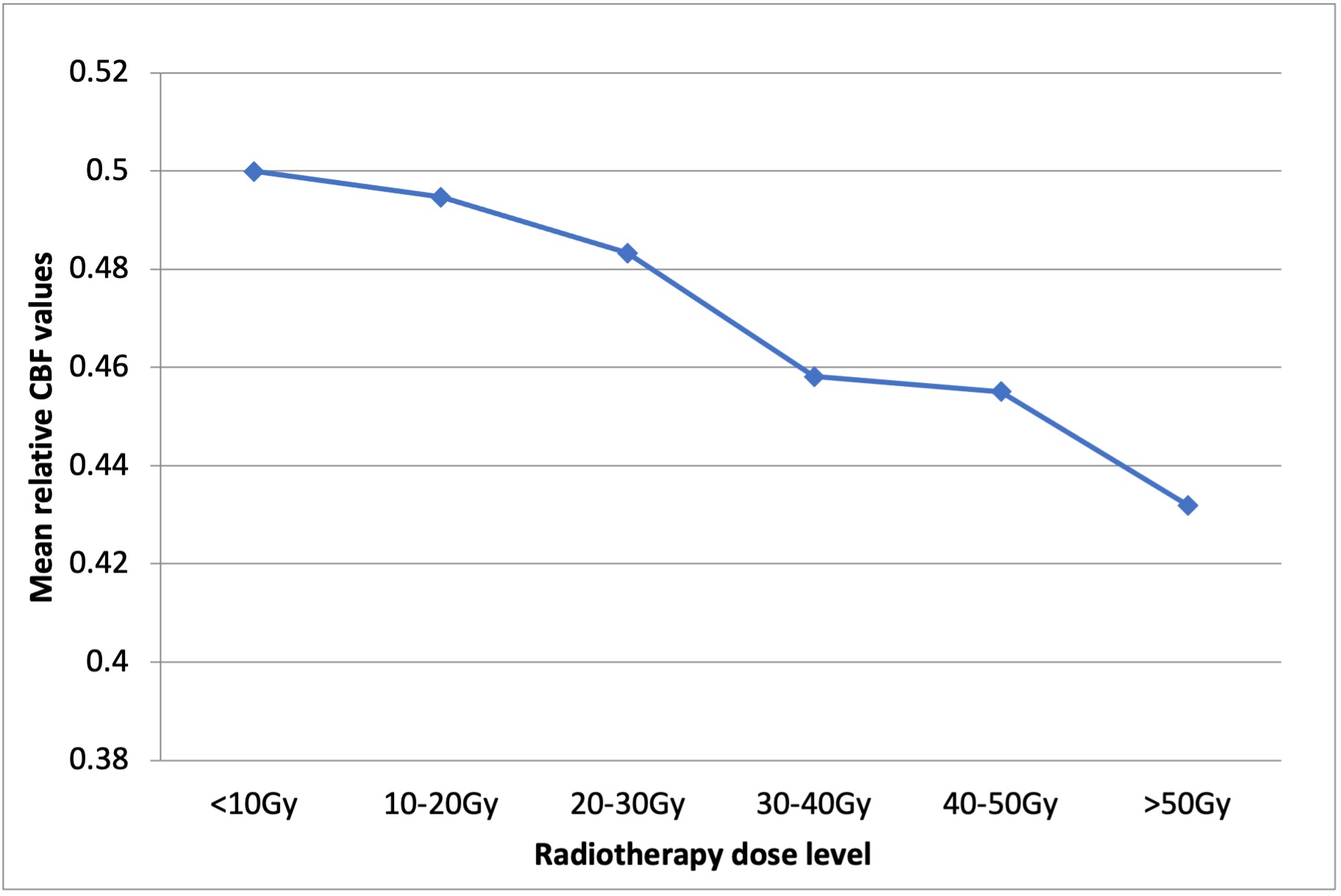
Testing of the function of the proposed framework outlined above was undertaken on a cohort of five randomly chosen patients. ASL perfusion data from these five patients shows a dose-dependent reduction in cortical perfusion outside the target volume, with a reduction in mean relative CBF values from 0.4999 at the lowest radiation doses (<10Gy) to 0.4319 at doses >50Gy (Figure 2).
Conclusion
A robust data framework for combining ASL perfusion data with RT dosimetric data has been developed. Early data indicate that reductions in grey matter CBF persist outside the target volume over one year after RT for glioma, and are dose dependent. This has implications for radiotherapy planning and post-treatment toxicity surveillance and potentially its management. Further analysis of the full patient cohort will be undertaken and available for presentation.