AI-based online adaptive CBCT-guided radiotherapy for bladder cancer using SIB and fiducial markers
Sana Azzarouali,
The Netherlands
PD-0235
Abstract
AI-based online adaptive CBCT-guided radiotherapy for bladder cancer using SIB and fiducial markers
Authors: Sana Azzarouali1, Karin Goudschaal1, Duncan den Boer1, Jorrit Visser1, Maarten Hulshof1, Arjan Bel1
1Amsterdam UMC, Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Accurate
external beam radiotherapy of the bladder with a simultaneous integrated focal
boost (SIB) is challenging due to variable bladder filling. With daily online
adaptation of the GTVs and OARs using AI-driven Cone Beam CT (CBCT)-guided
radiotherapy, we aim to reduce toxicity while maintaining target coverage. The
purpose of this is study is to analyze the workflow in the presence of fiducial
markers and to further enhance the accuracy of the boost dose on the tumor.
Material and Methods
Five patients
with muscle invasive bladder cancer were treated on a ring-based linac
integrated with a CBCT and software platform for both treatment planning and
delivery (Ethos, Varian, USA). In 20 fractions the bladder and first lymph
nodes received a dose of 40 Gy combined with a SIB of 15 Gy to the tumor.
Fiducial markers were used in four patients. Two pretreatment CT images were
made at t = 0 and t = 15 min. The first planning CT was used for manual delineation
and to make a reference plan (VMAT, 6MV FFF). A PTV margin of 7 mm was used,
but patient specifically extended in those directions where the PTV did not
cover the complete bladder on second pretreatment CT due to intrafraction
bladder filling . During each fraction a synthetic CT scan (sCT) was produced
by deformable registration of the planning CT to the CBCT. A structure set based
on the anatomy of the day was generated by using deformable registration and a
convolutional neural network. Manual corrections to the target structure were
performed if necessary, after which a scheduled plan was generated by
calculating the dose of the reference plan on the sCT. Subsequently, an adapted
plan was generated by running a new optimization. A second CBCT was acquired
for position verification prior to delivery. To evaluate the fraction and whether
the bladder was covered by the PTV, a post-treatment CBCT was acquired. The
duration of each step, manual corrections, planning decisions, intrafractional
bladder filling and target coverage were monitored.
Results
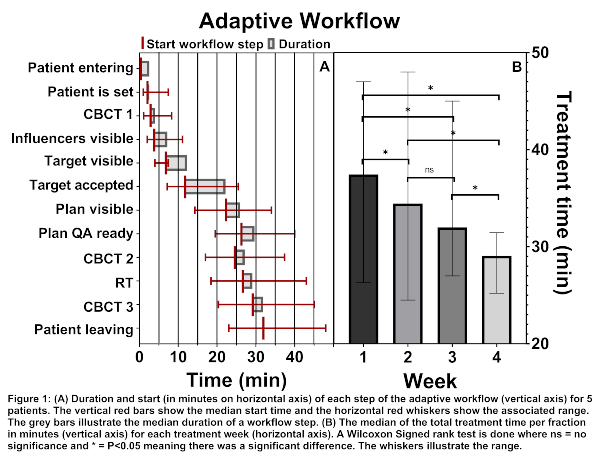
The
median treatment time was 32 min (Fig. 1A). For each week the treatment time
was significantly lower than the week before except for week 3 demonstrating
the presence of a learning curve (Fig. 1B). Compared to the fully automatic
workflow, an additional 5 min was needed if manual corrections were done.
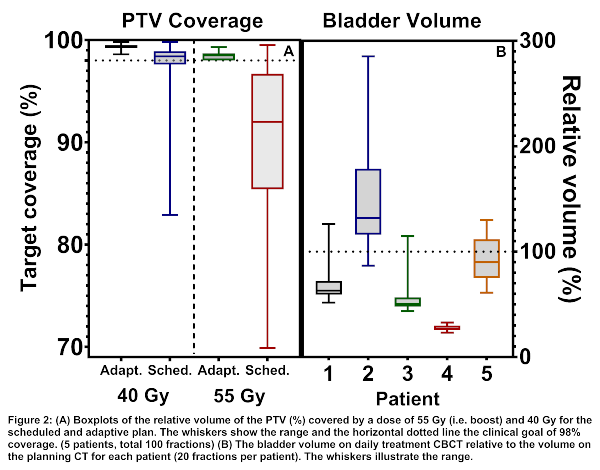
Manual corrections were made in 77% of all fractions. The adaptive plan was
used in 99% of all fractions. For the adaptive and scheduled plan 100% and 60%
of the cases resulted in a PTV V95>98%, respectively (Fig. 2A). The bladder
was covered by the PTV on CBCT3 in 87% of the fractions (Fig. 2B). In the other
13% a median of 0.9 cm of the bladder was outside the PTV due to intrafractional
bladder filling.
Conclusion
This study
shows that daily online adaptive CBCT-based RT with SIB is feasible for bladder
cancer. However, the workflow would benefit from a shortening of the
calculation time and lowering the need for manual corrections to reduce the
effect of intrafractional bladder filling.