Impact of respiratory motion for breast cancer proton therapy in free breathing
Line Bjerregaard Stick,
Denmark
PD-0231
Abstract
Impact of respiratory motion for breast cancer proton therapy in free breathing
Authors: Line Bjerregaard Stick1,2, Maria Fuglsang Jensen1, Camilla Jensenius Skovhus Kronborg1, Ebbe Laugaard Lorenzen3, Hanna Rahbek Mortensen1, Petra Witt Nyström1,4, Stine Elleberg Petersen5, Pia Randers5, Linh My Hoang Thai5, Esben Svitser Yates6, Birgitte Vrou Offersen5,6,7
1Aarhus University Hospital, Danish Centre for Particle Therapy, Aarhus, Denmark; 2Rigshospitalet, University of Copenhagen, Department of Oncology, Copenhagen, Denmark; 3Odense University Hospital, Laboratory of Radiation Physics, Odense, Denmark; 4Genetics and Pathology, Uppsala University, Department of Immunology, Uppsala, Sweden; 5Aarhus University Hospital, Danish Centre of Particle Therapy, Aarhus, Denmark; 6Aarhus University Hospital, Department of Oncology, Aarhus, Denmark; 7Aarhus University Hospital, Department of Experimental Clincial Oncology, Aarhus, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Today,
proton therapy for breast cancer is mostly performed in free breathing as
breathing motion is assumed to have minor impact on the radiological path
length when using an en face field
arrangements. This study examines the effect of respiratory motion in patients
with breast cancer receiving loco-regional proton therapy based on 4DCT scans.
Material and Methods
Twenty-five
patients with breast cancer (20 left-sided, five right-sided), treated at
Danish Centre for Particle Therapy in 2019 and 2020, were included. Patients
were immobilised in supine position with arms above the head. A planning CT
scan in free breathing and a 4DCT scan, both with 2 mm slice thickness, were
acquired for all patients on a Siemens Somatom Definition
Edge scanner. The
4DCT scan was sorted in ten phases according to amplitude. Breast or chest
wall, internal mammary nodes (IMN), interpectoral nodes and level 1-4 lymph
nodes (level 1 irradiation was required for 15 patients) were contoured as clinical
target volumes (CTVs) on the planning CT following the ESTRO guidelines. Relative
biological effectiveness (RBE) was fixed at 1.1. Patients were prescribed
either 40 Gy RBE in 15 fractions (nine patients) or 50 Gy RBE in 25 fractions
(16 patients). Clinical planning objectives: CTV breast/chest wall V95%
(relative volume receiving 95% of the prescribed dose) and CTV lymph nodes V90%
should be at least 98%. Spot-scanning proton therapy plans using two to three en face fields, single-field optimisation
and range shifter were created in Eclipse v13.7 (Varian Medical Systems). CTVs
were robustly optimised using 14 scenarios: 0 mm ±3.5% and ±5 mm ±3.5%.
The plan was recalculated on all ten phases of the 4DCT scan with fixed monitor
units. All ten phases in the 4DCT scan were deformable image registered to the
planning CT in Velocity v4.0 (Varian Medical Systems), and the deformed doses
from the phases were accumulated on the planning CT. A paired, two-tailed
Wilcoxon signed-rank test was used to compare dose metrics from the nominal
plan and the 4D evaluation.
Results
The median (range) amplitude of respiratory
motion measured at sternum position in the axial plane on the 4DCT scan was 2 mm
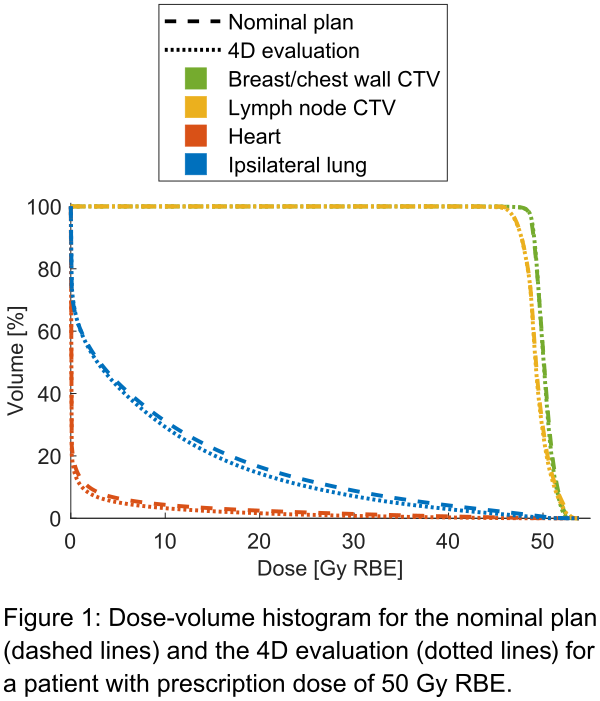
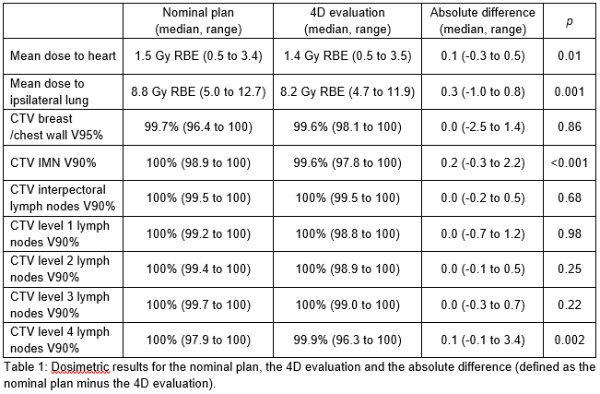
(1 to 4 mm). Dosimetric results from the nominal plan and the 4D evaluation can
be seen Table 1 and an example of a dose-volume histogram for a patient can be
seen in Figure 1. CTV coverage was below 98% for level 4 in one nominal plan and
three 4D evaluations, for IMN only in one 4D evaluation and for breast/chest
wall in one nominal plan. In the 4D evaluation, mean dose to the heart
increased to 0.3 Gy RBE (from 1.9 to 2.2 Gy RBE) and decreased to 0.5 Gy RBE (from
1.6 to 1.1 Gy RBE), and mean dose to the ipsilateral lung increased to 1.0 Gy
RBE (from 9.8 to 10.8 Gy RBE) and decreased to 0.8 Gy RBE (from 12.7 to 11.9 Gy
RBE).
Conclusion
Respiratory
motion has a modest impact on the dose distribution in proton therapy plans for
breast cancer when using robust and single-field optimisation and an en face beam arrangement.