Cardiac conduction system exposure during modern radiation therapy for mediastinal Hodgkin lymphoma
PD-0175
Abstract
Cardiac conduction system exposure during modern radiation therapy for mediastinal Hodgkin lymphoma
Authors: Pierre Loap1, Alfredo Mirandola2, Ludovic De Marzi1, Amelia Barcellini2, Viviana Vitolo2, Alberto Iannalfi2, Remi Dendale1, Ester Orlandi2, Youlia Kirova1
1Institut Curie, Department of Radiation Oncology, Paris, France; 2Centro Nazionale di Adroterapia Oncologica, Radiation Oncology Clinical Department, Pavia, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Radiation-induced
arrhythmias and conduction disorders are frequent adverse events of mediastinal
Hodgkin lymphoma radiotherapy. Exposition of cardiac conduction system during
mediastinal Hodgkin lymphoma (HL) radiotherapy has never been studied, despite
increasing use of volumetric modulated arc therapy (VMAT) which tends to expose
larger volume to low dose bath. We evaluated conduction node exposure during mediastinal
HL irradiation with VMAT and estimated the potential dosimetric benefit with
intensity modulated protontherapy (IMPT).
Material and Methods
Atrioventricular
(AVN) and sinoatrial (SAN) nodes were retrospectively delineated according to published
guidelines on the simulation CT scans of 20 localized unfavorable mediastinal
HL cancer patients treated in a consolidative setting with deep-inspiration
breath-hold (DIBH) VMAT. IMPT treatment was re-planned on the simulation CT
scans. Mean and maximum doses to the SAN and to the AVN were retrieved and
compared. Correlation coefficients were calculated between doses to the SAN, to
the AVN and to the whole heart.
Results
For VMAT
irradiation, the SAN mean dose was 7.0 Gy [range: 0.0-24.3 Gy] and the SAN maximum
dose was 13.2 Gy [0.2-29.4 Gy]; the AVN mean dose was 2.1 Gy [0.0-16.7 Gy] and
the AVN maximum dose was 2.7 Gy [0.0-19.4 Gy].
IMPT significantly reduced SAN mean dose to 1.7 Gy [0.0-11.1 Gy]
(p<0.01), SAN maximum dose to 5.5 Gy [0.1-25.8 Gy] (p<0.01), AVN mean
dose to 0.1 Gy [0.0-1.1 Gy] (p<0.01), and AVN maximum dose to 0.2 Gy
[0.0-2.8 Gy] (p<0.01) (Figure 1). For VMAT, correlations were strong between
mean doses to the heart and to the SAN (r=0.85) and between mean doses to the
heart and to the AVN (r=0.94); they were moderate between maximum doses to the
heart and to the SAN (r=0.63) and weak between maximum doses to the heart and
the AVN (r=0.38). After IMPT replanning, correlations became moderate between
mean doses to the heart and to the SAN (r=0.64) but remain strong between mean
doses to the heart and to the AVN (r=0.86); they became unsignificant between maximum
doses to the heart and to the SAN (r=0.24) and remained weak between maximum
doses to the heart and to the AVN (r=0.31).
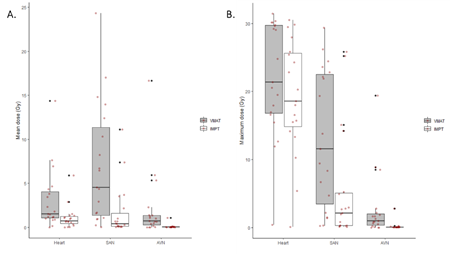
Figure 1:
Cardiac conduction node exposure during mediastinal Hodgkin lymphoma
irradiation with volumetric modulated arc therapy (VMAT) or intensity modulated
proton therapy (IMPT) with deep-inspiration breath-hold (DIBH). Mean (A) and maximum (B) doses delivered to the heart, to the
sino-atrial node (SAN) and to the atrio-ventricular node (AVN).
Conclusion
The
SAN can be substantially exposed during mediastinal HL radiotherapy with DIBH-VMAT.
Mean heart dose is poorly representative of conduction node exposure. Proton
therapy significantly reduces radiation doses to the cardiac conduction system
and might consequently be considered in case of underlying rhythmic or
conduction disorders.