Multi-parameter patient selection strategy for Hodgkin lymphoma proton therapy
PD-0172
Abstract
Multi-parameter patient selection strategy for Hodgkin lymphoma proton therapy
Authors: Pierre Loap1, Alfredo Mirandola2, Ludovic De Marzi1, Amelia Barcellini2, Viviana Vitolo2, Alberto Iannalfi2, Remi Dendale1, Youlia Kirova1, Ester Orlandi2
1Institut Curie, Department of Radiation Oncology, Paris, France; 2Centro Nazionale di Adroterapia Oncologica, Radiation Oncology Clinical Department, Pavia, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Hodgkin
lymphoma (HL) is a highly curable hematological neoplasia. Consolidation
radiation therapy techniques have made significant progresses to reduce late
radiation-induced toxicity. Recent technical breakthroughs notably include
intensity modulated proton therapy (IMPT), which has demonstrated a major
dosimetric benefit at the cardiac level for mediastinal HL patients. However,
its implementation in clinical practice is still challenging due to the current
shortage of proton therapy facilities and the increased cost of this technique.
In this context. The purpose of this study is to propose a general frame for
mediastinal HL patient selection strategy for IMPT, taking into account patient
clinical characteristics and overall IMPT treatment availability.
Material and Methods
We
included 20 HL patients treated with VMAT. IMPT plans were generated on initial
simulation scans. Dose to the heart, to the left ventricle and to the valves
were retrieved to calculate the relative risk (RR) of ischemic heart disease
(IHD), congestive heart failure (CHF) and valvular disease (VD). Composite
relative risk reduction (cRRR) of late cardiotoxicity between IMPT and VMAT
were calculated as weighted means of relative risk reduction for IHD, CHF and
VD, across a wide range of cardiovascular risk factors, using the initial RR
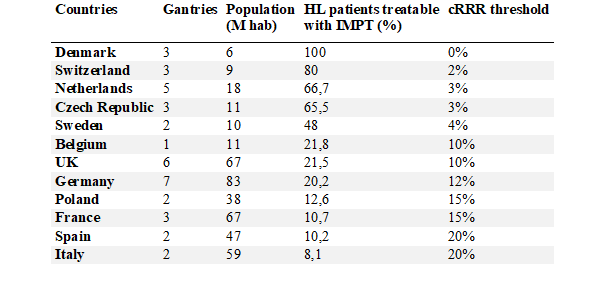
with VMAT as ponderations factors. The proportion of mediastinal HL patients
who could benefit from IMPT was estimated in European countries, based on the
population and the number of active gantries, to propose country-specific cRRR
threshold for patient selection.
Results
Twenty
patients were treated between January 2018 and May 2020 at Institut Curie
(Paris, France). Compared with VMAT, IMPT significantly reduced mean dose to
the heart (1.79 Gy vs 0.88 Gy, p<0.01), to the left ventricle (0.59 Gy vs
0.02, p<0.01) and to the valves (1.36 Gy vs. 0.03, p<0.01). For a HL
patient without cardiovascular risk factor treated with anthracycline, the
relative risks of late cardiovascular complication were significantly higher
after VMAT compared with IMPT for ischemic heart disease (median 1.13 vs. 1.07,
p<0.01), for congestive heart failure (2.98 vs. 2.84, p=0.01), and for
valvular disease (1.03 vs. 1.01, p=0.05). Considering all possible combination
of cardiovascular risk factor, the median cumulative relative risk reduction
(cRRR) with IMPT was 4.2%, ranging between 0.1% and 30.3%. The estimation of
the proportion of HL patients currently treatable with IMPT in European
countries (with proton therapy centers) ranged between 8% for Italy and 100%
for Denmark, corresponding to cRRR threshold between 20% and 0%.
Conclusion
This multi-parameter selection strategy for HL
protontherapy, taking simultaneously into consideration patient clinical
characteristics and national treatment capacity, allows flexible patient
selection in case of IMPT availability shortage and might be readily
implemented for other tumor types.