3D MRI versus conventional ultrasound tumour measurements for treatment planning of eye tumours
Lisa Klaassen,
The Netherlands
PD-0075
Abstract
3D MRI versus conventional ultrasound tumour measurements for treatment planning of eye tumours
Authors: Lisa Klaassen1,2,3, Myriam Jaarsma-Coes2,1, Teresa Ferreira2, Khanh Vu1, Marina Marinkovic4, Gregorius Luyten1, Coen Rasch3, Jan-Willem Beenakker1,2,5
1Leiden University Medical Center, Ophthalmology, Leiden, The Netherlands; 2Leiden University Medical Center, Radiology, Leiden, The Netherlands; 3Leiden University Medical Center, Radiation Oncology, Leiden, The Netherlands; 4Leiden University Medical Center, Ophthalmology, Leide, The Netherlands; 5Leiden University Medical Center, Radiation Oncology, Leiden, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Uveal melanoma (UM) is the most frequently
occurring malignant primary eye tumour. Ocular MRI, enabling 3D tumour imaging
and providing a better soft tissue contrast than conventional 2D ultrasound
(US), is increasingly used for the diagnosis, therapy planning and follow-up of
UM. Tumour prominence (thickness) and largest basal diameter (LBD) are the
primary determinants for the brachytherapy applicator size and application time
and are used to define the 3D clinical target volume in proton beam therapy.
Within this study, we aim to compare US and MRI dimension measurements and
determine the most suitable measurement modality.
Material and Methods
Data of 25 UM patients with a wide range in size
and location were analysed retrospectively. Patients were scanned at 3 Tesla
MRI according to the protocol of Ferreira (Cancers 2019). The tumour was
semi-automatically delineated on the contrast-enhanced T1-weighted images
(acquisition voxel size 0.8x0.8x0.8 mm3) in MevisLab.
The prominence and LBD were automatically
obtained from the MRI contours. MRI measurements were compared to the clinical
US measurements (resolution 0.4 mm) and related to tumour location in the
anteroposterior direction. Tumours where the measurement did not fit into the
US field of view (FOV) or where the extent of flat tumour components was
difficult to assess on MRI were assessed separately.
Results
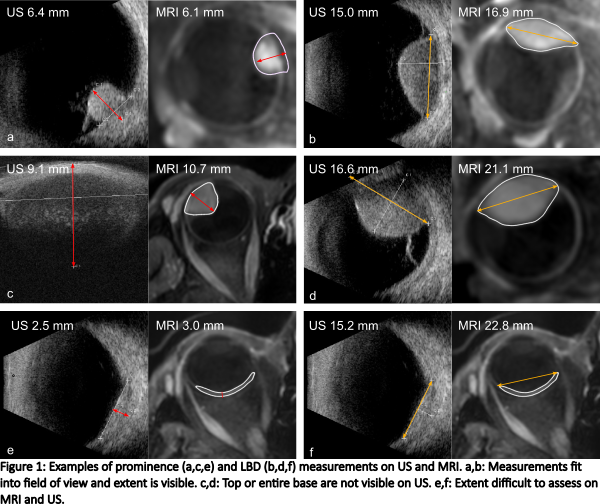
For 7/25 patients, the prominence and/or LBD
measurement did not fit into the US FOV. All these tumours were located in the
anterior 50% of the eye. Of the 4 patients with an US prominence <4 mm,
tumour extent was difficult to assess on MRI for 3/4 (Fig 1).
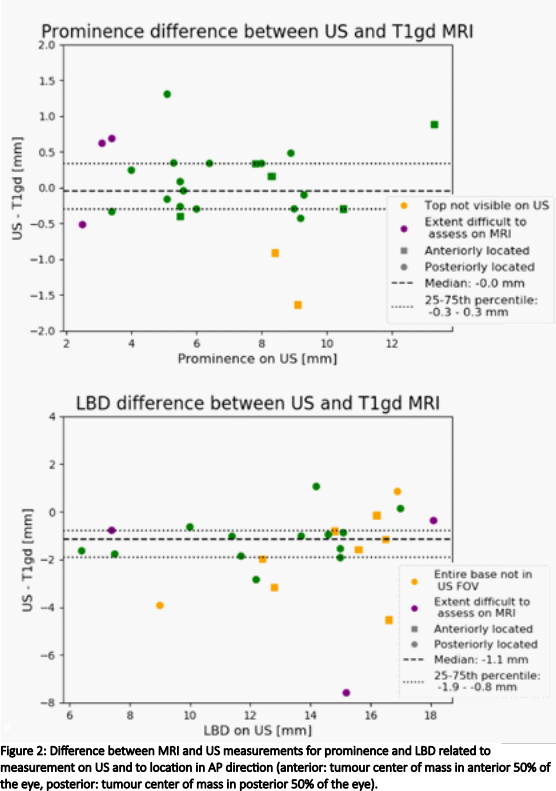
When tumour extent was visible on both imaging
modalities, median absolute differences were 0.3 mm (range 0.0-1.3 mm) for
prominence and 1.1 mm (range 0.1-2.8 mm) for LBD, respectively (Fig 2). For the
LBD, 80% of measurements was more than 0.5 mm larger on MRI. For patients for
whom the tumour extent was difficult to assess on one imaging modality, the
median absolute difference for the prominence and LBD were 0.7 mm (range
0.5-1.6 mm) and 1.4 mm (range 0.1-7.6 mm).
Conclusion
MRI and US yield similar prominence
measurements (median absolute difference 0.3 mm) when tumour extent is visible on
both modalities. However, in anteriorly located tumours, MRI measurements are
more accurate, and using US for these tumours might lead to an underestimation of
tumour diameter, possibly due to difficulty correctly positioning the
ultrasound transducer. The extent of flat tumours can be difficult to assess on
MRI, although, the distinction between tumour and healthy tissue may not be
evident on US either. For these tumours, tumour measurements may be supported
by fundoscopic imaging.