Determination of the optimal nadir PSA following partial gland ablation in prostate brachytherapy
MO-0299
Abstract
Determination of the optimal nadir PSA following partial gland ablation in prostate brachytherapy
Authors: Ben Vanneste1, Vassilios Skouteris2, Luis Campos Pinheiro3, Richard Stock4, Nelson Stone5
1MAASTRO, Radiation Oncology, Maastricht, The Netherlands; 2Hygeia Hospital, Urology, Athens, Greece; 3Hospital da Luz,, URology, Lisboa, Portugal; 4 The Icahn School of Medicine at Mount Sinai , Radiation Oncology, New York, USA; 5The Icahn School of Medicine at Mount Sinai New York, Urology and Radiation Oncology , New York, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Patients are seeking less invasive
therapies when diagnosed with localized prostate cancer. Determination of a
successful ablation of the clinical treatment volume (CTV) relies on knowledge
of the new or nadir PSA (nPSA) following the ablation. We propose a novel
method of determining this value.
Material and Methods
The nPSA can be derived from the contribution
of PSA from the prostatic epithelium (benign and cancer) of the treated (CTV) and
the untreated volume. We calculated the contribution of PSA from the CTV by
analyzing a cohort of 2861 men treated with prostate brachytherapy (PB) of
which 2064 (72%) were without Phoenix failure Phoenix failure and were followed
> 5 years. Delivered doses was converted to the biologically
effective dose (BED) using the post-implant D90 and any external beam boost
with an α/β of 2. BED levels of < 150, >
150-200 and > 200 Gy were compared to a last PSA <0.2 ng/ml by
ANOVA from the PB database. Secondly, the PSA was determined for untreated
non-cancerous prostate volume by analyzing another cohort of patients. 123
(55.1%) of 243 men with clinical suspicion of prostate cancer who underwent transperineal
mapping biopsy and were found to have only benign pathology (no cance). PSA values for the men with
benign disease were analyzed in 4 percentile groups for their PSAD (PSA
density) values. Regression analysis with a linear model was used to determine which
group had the highest R2 value. An equation was constructed to
determine the nPSA for a patient treated with partial gland ablation.
Results
For
the first cohort, with a mean follow-up of 11.3 years (range 5-24) the last
mean PSA for the non-failures were 0.14, 0.08 and 0.05 ng/ml (p<0.001) for
the 3 BED groups. The percent of men with a PSA < 0.2 was 82.8, 93.1 and
96.8%, respectively. For the second cohort of patients with a benign biopsy mean
age, PSA, PSAD, prostate volume (PV) and number of biopsy specimens taken were:
64.8 years, 7.6 ng/ml, 0.15, 54.6 cc and 45. Mean PSAD for the 4 percentiles
ranged from 0.117-0.12 (p<0.001). The optimal PSAD (highest R2)
for men without prostate cancer was 0.12
ng/ml2 (figure 1). For men receiving a partial implant to the CTV where
the delivered dose had a BED of > 200 Gy (I-125 post-implant D90 > 189
Gy), the PSA contribution of the treated volume would be < 0.2 ng/ml,
and the PSA contribution of the remaining benign prostate could be calculated
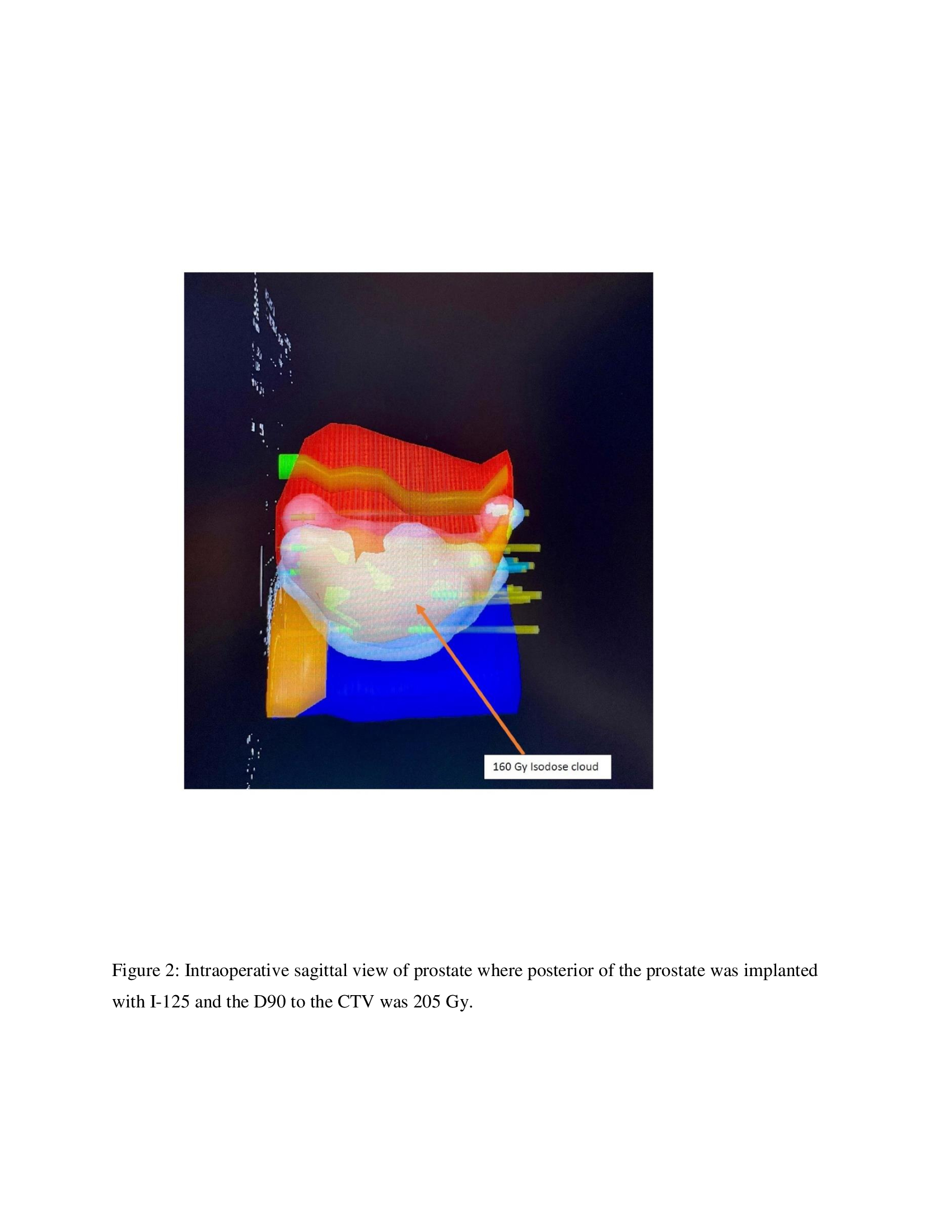
as: pretreatment PV (cc) – CTV (cc) x
0.12. For example, the nPSA of a recent patient with a PV of 42 cc implanted
with I-125 to the CTV of 18 cc which received a D90 of 205 Gy should reach (42-18)
x 0.12 = 2.88 ng/ml (figure 2).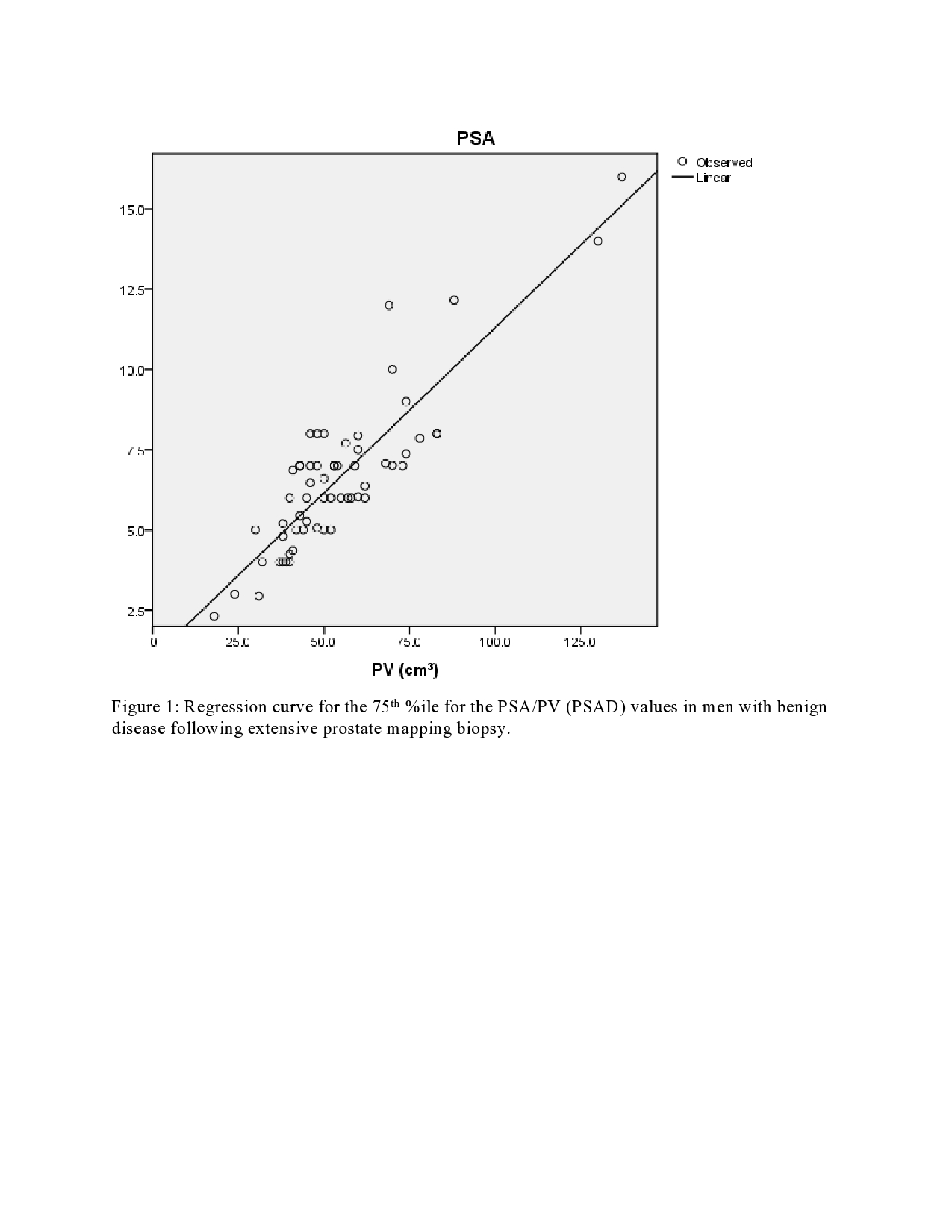
Conclusion
We proposed a simple method for determining
the new nadir PSA following partial gland ablation. This formula assumes the
treated portion of the gland would be not produce any PSA after receiving an
ablative dose of radiation. The remaining benign gland should generate a nPSA 0.12
times the untreated prostate volume. Further validation of this concept is
warranted.