Optimization of adaptive aperture to improve organs at risk sparing in proton therapy
Marta Bogowicz,
The Netherlands
MO-0636
Abstract
Optimization of adaptive aperture to improve organs at risk sparing in proton therapy
Authors: Marta Bogowicz1, Vicki Taasti1, Mirko Unipan1, Geert Bosmans1, Phil Broussard2, Wouter van Elmpt1
1GROW School for Oncology, Maastricht University Medical Centre+, Department of Radiation Oncology (Maastro), Maastricht, The Netherlands; 2Mevion Medical Systems, Inc, Littleton, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
The adaptive aperture (AA) is a unique feature
of Mevion Hyperscan S250i proton beam delivery system. In contrary to a static
aperture, the AA allows for dynamic trimming of the proton beam (e.g. similar
to a photon MLC) with the shape of AA adjusted for every energy layer. In its
current implementation, only one AA setting per energy layer is available. As a
consequence, only spots on the edge of the spot map are trimmed. Trimming of
the inner spots could be beneficial in systems with relatively big spot sizes. Here we
investigated the added value of a forward AA optimization to create steeper
lateral dose fall-off and show the potential for reduction of organs at risk (OARs)
dose.
Material and Methods
The simulation part of the study was conducted
using single treatment beam and a numerical phantom (simulated water tank with
10x10x1cm CTV at 4.8cm depth and OARs of 10x2x1cm placed on the side of the
CTV, with CTV-OAR distance ranging from 0 to 10mm). The clinical investigation included
three patients with brain tumors, with variable location within the brain. Treatment
plans were created in RayStation v10A.
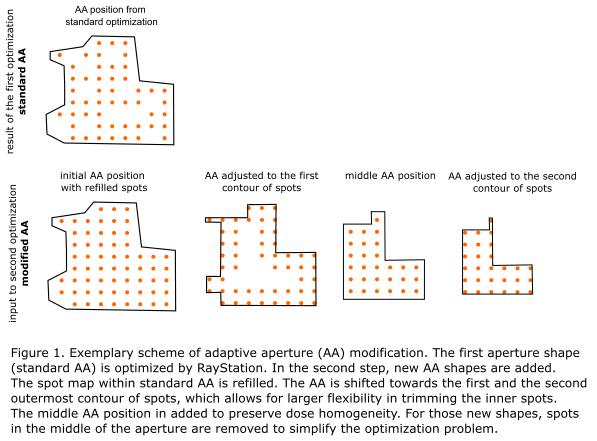
First,
a plan was optimized with standard AA settings according to clinical protocol,
using robust optimization with 1mm setup and 3% range uncertainty. Next, three
additional AA positions were added per energy layer using RayStation scripting.
To create the new AA shapes, original AA was shifted towards the field center,
so that it closely followed the first and the second outermost contour of the
spots (Fig 1). Finally, the modified AA plans were reoptimized and objectives
were adjusted if needed to ensure a clinically acceptable plan. The plans were
evaluated for their robustness computing voxel-wise minimum and maximum (VWmin/max)
dose distributions. The CTV coverage was analyzed in VWmin, the D0.03cc in
VWmax and mean doses in the nominal dose distribution. For the clinical cases, the
reduction in 80% isodose between standard AA and modified AA plans was evaluated.
Results
In the phantom study, the lateral beam penumbra
was reduced by 2.6mm (from 10.3mm to 7.7mm). Furthermore, relevant reduction of
dose to simulated OARs was observed. Reduction in mean dose to OARs was around 7%
of the prescribed dose. Reduction in D1% ranged from 0% to 16% and was larger for
the OARs at larger CTV-OAR distance.
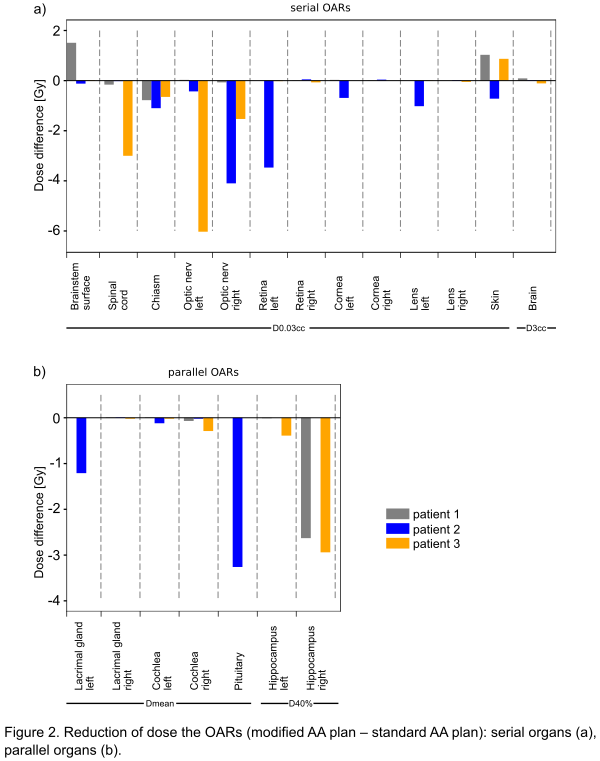
For all 3 clinical cases, CTV coverage remained
comparable to the standard AA plan. The modified AA plans resulted in reduction
of dose to all OARs (Fig 2) with the exception of small increase of D0.03cc to brainstem
and skin. However, this increase was below 1.5Gy and remained within the OAR
tolerance. For every patient, at least one OAR had dose reduction >2Gy. Volume
of isodose 80% (normalized to CTV volume) decreased by 16%, 12% and 44% for
patients 1, 2 and 3, respectively.
Conclusion
This
study presented a proof of concept describing the optimization of AA. The lateral
dose fall-off was improved and led to clinically relevant reduction in OAR
doses with preserved CTV coverage.