First clinical results of integrated EMT for quantification of positional deviations in cervix BT
Inger-Karine Kolkman-Deurloo,
The Netherlands
OC-0278
Abstract
First clinical results of integrated EMT for quantification of positional deviations in cervix BT
Authors: Inger-Karine Kolkman-Deurloo1, Jeremy Schiphof-Godart1, Laura Heerden van1, Gonnie Erp van1, Miranda Christianen1, Jan-Willem Mens1, Renée Rijnsdorp1, Lorne Luthart1, Remi Nout1, Mischa Hoogeman1
1Erasmus MC Cancer Institute, Radiotherapy, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
For correct dose delivery in cervix brachytherapy
(BT) the dwell positions and times need to precisely correspond to the
treatment plan. Correspondence of the actual applicator and needle positions
with the MRI/CT-based treatment plan is therefore essential. Positional
deviations however might occur due to applicator and/or needle shifts, transfer
tube swaps, anatomical changes or reconstruction uncertainties. Electromagnetic
tracking (EMT) has been proposed for detection of such errors and uncertainties.
The feasibility of EMT using a prototype of a hybrid EMT/BT system, i.e. a
Flexitron afterloader with an EMT sensor integrated in the check cable (Elekta,
Veenendaal) has previously been demonstrated by phantom experiments in typical
clinical BT environments. An accuracy of less than a millimeter was found in 6F
interstitial plastic needles. The purpose of this study is to prospectively analyze
the feasibility of this system to detect treatment errors and reconstruction
uncertainties in cervix HDR BT patients.
Material and Methods
Twenty cervix patients, treated with three or four HDR
BT fractions using an intracavitary/interstitial applicator as part of their
treatment, were included in a prospective study, simulating a workflow with EMT-based
treatment verification. EMT measurements, scheduled before dose delivery in one
to three BT fractions per patient, were performed using the hybrid EMT/BT
afterloader by automatically moving the EMT sensor through all needles in the
implant according to a predefined MRI- or CT-based treatment plan. Dose
delivery was performed afterwards using our clinical afterloader, ensuring that
the clinical treatment was not affected by the EMT experiments. The intracavitary channels were discarded in
this study as our phantom study showed unacceptable deviations. The residual errors, i.e., the Euclidean
distances between the registered EMT measured and planned dwell positions, were
calculated.
Results
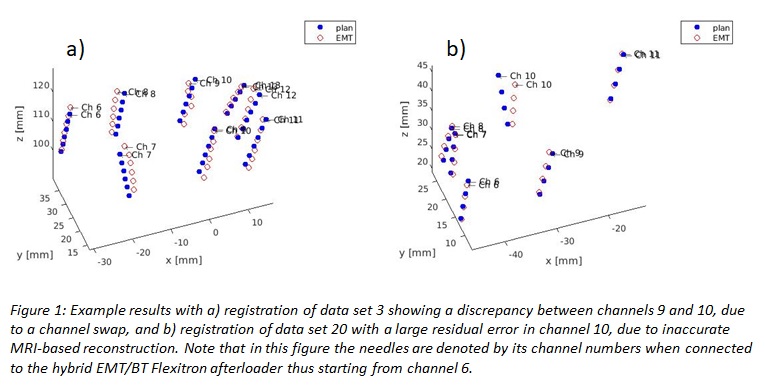
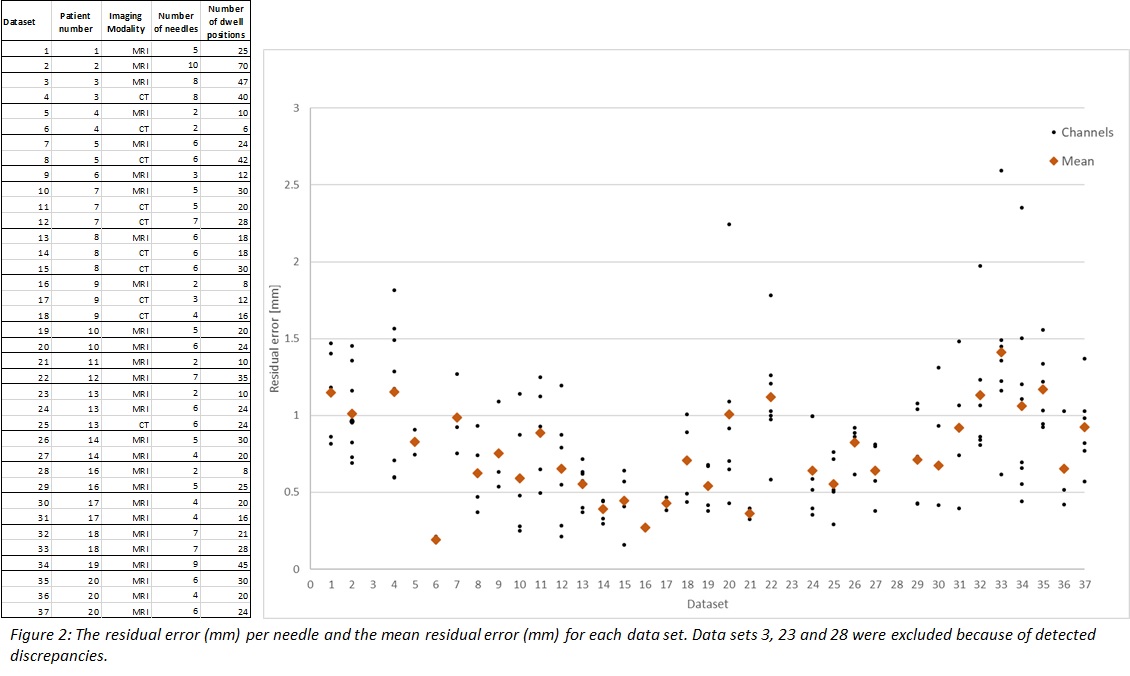
Data sets from 37 fractions were available for
analysis. In three data sets (3, 23 and 28) a discrepancy between the
registered EMT and planned dwell positions, e.g. a channel swap (fig. 1a), was
detected. The increased difficulty in needle reconstruction based on MRI scans
compared to CT scans was reflected by a significant difference in mean residual
error (p<0.001), i.e. 0.90 mm and 0.68 mm for MRI-based and CT-based reconstruction,
respectively. Moreover, outliers were detected in 5 data sets (20, 22, 32, 33
and 34), i.e., a single needle with a high residual error. These datasets were all
planned using MRI and contained ≥ 6 needles, again suggesting reduced reconstruction
accuracy for MRI (fig. 1b). The results are summarized in figure 2.
Conclusion
This
study demonstrates that the hybrid EMT/BT system can detect treatment errors and
needle reconstruction inaccuracies in HDR BT cervix patients in a clinical
setting.