Systematic multi-disciplinary sequence evaluation for integration into the MR-linac workflow
Sophie Alexander,
United Kingdom
MO-0312
Abstract
Systematic multi-disciplinary sequence evaluation for integration into the MR-linac workflow
Authors: Sophie Alexander1, Joan Chick2, Trina Herbert1, Robert Huddart3, Manasi Ingle3, Adam Mitchell2, Simeon Nill2, Uwe Oelfke2, Alex Dunlop2, Shaista Hafeez3
1The Royal Marsden NHS Foundation Trust, Radiotherapy, Sutton, United Kingdom; 2The Royal Marsden Hospital and the Institute of Cancer Research, Joint department of physics, Sutton, United Kingdom; 3The Royal Marsden Hospital and the Institute of Cancer Research, Uro-Oncology, Sutton, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Vendor-approved
Magnetic Resonance (MR) sequences are provided for MR-linac workflows however
alternative ‘off-label’ sequences may offer advantages. Prior to clinical use,
the safety, accuracy and overall clinical benefit should be determined. The aim
of this study was to develop a systematic approach for off-label sequence
evaluation and demonstrate the application for bladder cancer MR-guided
radiotherapy (MRgRT) on Unity (Elekta AB, Stockholm).
Material and Methods
Two T2-weighted
Turbo Spin Echo off-label sequences were proposed, denoted 1.1min3mm and 3.4min2mm,
indicating both acquisition time and slice thickness. Each sequence was
assessed against the vendor provided 2min1mm sequence.
The off-label sequences
were acquired during opportunity scanning time on 3 patients receiving daily bladder
cancer MRgRT, for up to 3 fractions per patient. Images were exported to Monaco
treatment planning system (TPS) for offline review (v5.40.1, Elekta). Microsoft
forms employing four-point Likert scales were created to guide qualitative
review of image quality and workflow suitability, carried out independently by
two doctors and two treatment radiographers.
Geometric
accuracy, image uniformity and ghosting were assessed using the ACR phantom
(acr.org). The impact of the larger slice thickness within the TPS included
assessment of margin expansions, optimisation behaviour and dosimetric impact (carried
out by physicists). Existing clinical bladder treatment image data (2min1mm)
were used in VolumeView (v5.3.31, Philips Medical Systems, Best) to reconstruct
2mm and 3mm slice thickness data sets for plan generation using the same
clinical template. Treatment plans were then recalculated on the corresponding
2min1mm sequence and were compared using clinical goals, and dose conformity.
To quantify the
potential reduction in overall treatment time for the shorter acquisition of
the 1.1min3mm sequence, a phantom treatment workflow was carried out.
Results
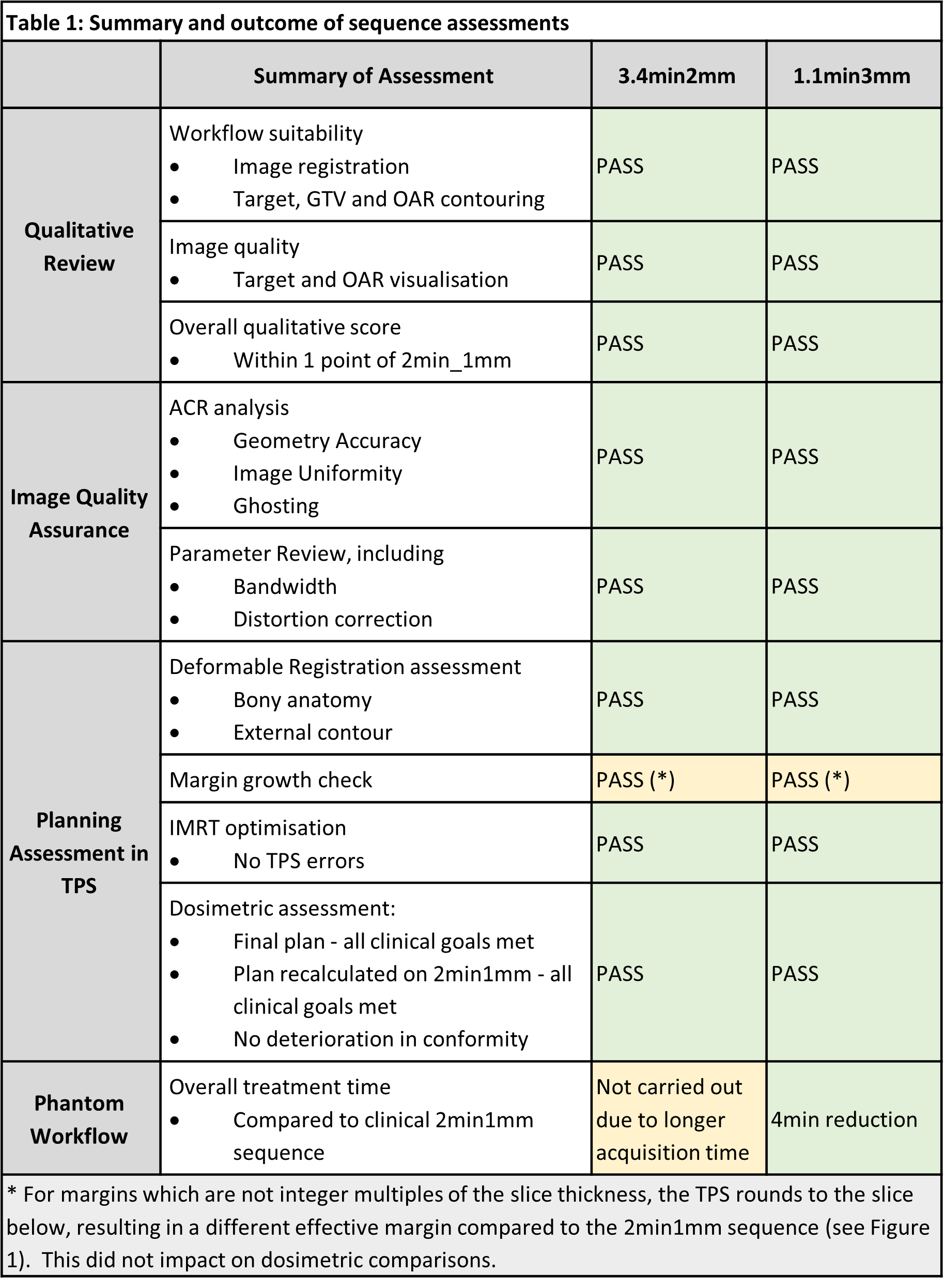
Table
1 summarises the results. Both sequences were shown to be accurate, safe and of
non-inferior utility to the 2min1mm sequence and facilitated clinically
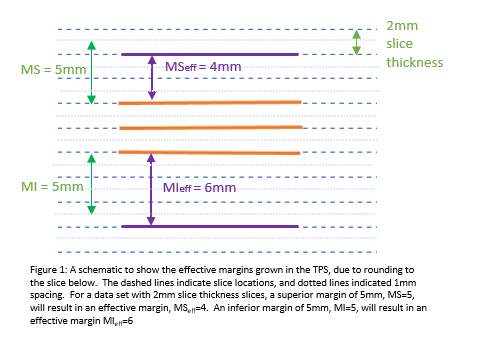
acceptable treatment plans in Monaco. For margins that are not integer multiples
of the slice thickness, the effective margin can differ (see Fig 1), however no
dosimetric impact was seen. The workflow time reduction of 4min for the
1.1min3mm sequence can be attributed to both shorter acquisition and reduced
dataset size. This could translate into a 14% time reduction to the average bladder
cancer MRgRT at our centre.
Conclusion
A systematic sequence
evaluation was developed and used to evaluate off-label sequences for use in bladder
MRgRT on the Unity MR-Linac. The use of the proposed 1.1mm3mm sequence will enable
meaningful reduction of the workflow time. This has potential to minimise intra-fraction
target volume changes and permit safe future PTV margin reduction. This
approach to evaluating off-label sequences will be applied to other indications
and sequences before clinical implementation.