One stop shop single fraction MR-guided stereotactic radiotherapy: Workflow and patient satisfaction
S. Verheijen,
The Netherlands
MO-0311
Abstract
One stop shop single fraction MR-guided stereotactic radiotherapy: Workflow and patient satisfaction
Authors: Sonja Verheijen1, Ruud de Moes2, Miguel A. Palacios2, Cornelis J.A. Haasbeek2, Famke L. Schneiders2, Anna M.E. Bruynzeel2, Berend J. Slotman2, Frank J. Lagerwaard2, Suresh Senan2
1Amsterdam UMC, VUmc location, de Boelelaan 1117, 1081 HV Amsterdam, Department of Radiation Oncology, Amsterdam, The Netherlands; 2Amsterdam UMC, location VUmc, de Boelelaan 1117, 1081 HV Amsterdam, Department of Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Single fraction SBRT is a standard treatment
option for lung malignancies. We report on the workflow and patient
satisfaction for a one stop shop (OSS) service for delivery of MR-guided SBRT in
lung tumors.
Material and Methods
Suitable patients were identified by a radiation oncologist before
consultation. Eligibility criteria were tumor size <5cm, located >1 cm
from critical structures, and tumor visibility on both a 3D MR scan and MR-cine
acquisitions. The workflow consisted of consultation, simulation, treatment
planning and delivery. The duration of each step was monitored. After SBRT, patients
completed a questionnaire to assess their overall impression with the OSS
procedure and waiting times between workflow steps.
A dedicated MR-simulation session assessed tumor mobility in
3 planes, in combination with a 3D MR scan in breath-hold, followed by a breath-hold
CT scan for dose calculation purposes. IMRT step-and-shoot plans were generated,
using typically 12 beams and 25 segments. The prescribed dose was either 30 or
34Gy to the PTV, in accordance with NRG-RTOG 0915 trial constraints. In a
second phase of the OSS procedure, autocontouring of OARs was implemented in combination
with the use of a patient-specific template for dose optimization derived from
a preplanning on a diagnostic CT. SBRT was delivered on an MR-linac, with breath-hold
gating performed using visual feedback of real-time tumor tracking on a video
screen. Online plan-adaptation enabled two consecutive sessions, allowing
patients to rest during treatment, thus increasing gating efficiency.
Results
Seven patients underwent the OSS procedure. All
treatment plans fulfilled institutional dose constraints. Figure 1A shows the
time spent by a patient in each workflow step. Total procedure time decreased from on
average 7.5h for the first 5 patients, to 4h for latter patients. Simulation took
45 min on average. Treatment planning times decreased from 4.0h to 1.2h after
implementation of auto contouring of organs at risk and the use of
patient-specific templates. Full breath-hold delivery and re-optimization took
on average 1.3hrs.
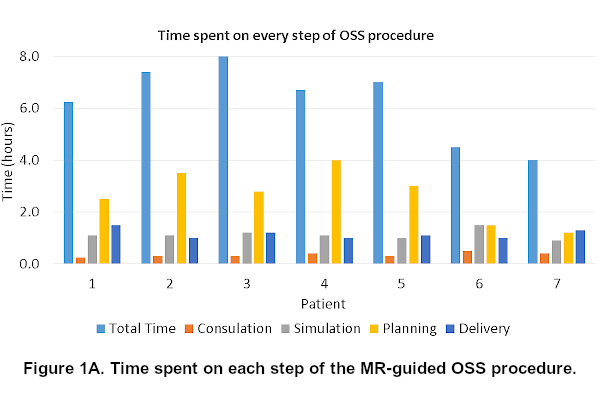
Figure 1B summarizes findings from patient questionnaires
completed at the end of the OSS treatment. All patients were pleased with the
opportunity to complete pre-treatment imaging and treatment in one single day. However,
some regarded the experience as somewhat taxing. A slightly lower satisfaction
was noted by three of the first 5 patients whose OSS procedure took >6.0h,
as they had to wait at least 3.0h between simulation and treatment.

Conclusion
A OSS MR-guided lung SBRT service was
successfully implemented. Patients preferred pre-treatment imaging and delivery
in one single day, and also appeared more satisfied with shorter stays at the
department. Measures to further shorten the workflow are being explored, and
use of the OSS implementation will extend to other tumor sites.