Quantifying individual dose relationships for pCR in rectal cancer: potentials for a customized dose
Alessandro Cicchetti,
Italy
MO-0880
Abstract
Quantifying individual dose relationships for pCR in rectal cancer: potentials for a customized dose
Authors: Alessandro Cicchetti1, Paolo Passoni2, Sara Broggi1, Najla Slim2, Antonella Del Vecchio1, Stefano Cascinu3, Francesco De Cobelli4, Riccardo Rosati5, Nadia Di Muzio2, Claudio Fiorino1
1San Raffaele Scientific Institute, Medical Physics, Milan, Italy; 2San Raffaele Scientific Institute, Radiotherapy, Milan, Italy; 3San Raffaele Scientific Institute, Oncology, Milan, Italy; 4San Raffaele Scientific Institute, Radiology, Milan, Italy; 5San Raffaele Scientific Institute, Gastroenterology Surgery, Milan, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
To develop a model for individual pathological Complete Response (pCR) prediction for rectal cancer patients (pts) treated with neo-adjuvant radio-chemotherapy (RCT). The suggested approach combines the classical Logit dose-effect curve with the individual early response assessed by MRI imaging during RCT.
Material and Methods
A population-averaged dose-effect curve for pCR may be derived by fitting published data: the recent meta-analysis by Hall et al. was utilized. Then, we considered data of 90 pts from our Institute treated with RCT in which a relationship between a previously introduced early regression index (ERI, assessed at half RCT) and pCR was quantified and found to be highly predictive. The index is proportional to the ratio of tumor volumes during and before RCT, with lower values indicating better response. ERI was considered as a dose modifying factor (DMF), "adapting" the resulting dose-effect curve to this population. The Logit curve assessed from the meta-analysis was first tuned on our population: the bivariate logistic pCR model was converted into a Logit EQD2 model with ERI acting as a dose modifying factor (DMF) for the estimated rate of pCR. The final model resulted in a series of sigmoid shaped curves, depending on individual ERI values. After successful fitting, the model was applied to quantify the expected increase of pCR with dose, depending on patient response.
Results
The resulting Logit model depending on the 2Gy-equivalent dose (EQD2) and ERI showed best-fit values of TD50 = 52.2 Gy, DMF = 0.017 x ERI + 0.89 the steepness m = 1/(3.7 + 0.07 x ERI). Of note, the meaning of TD50 coincides with the classical one (i.e.: the dose corresponding to pCR=50%) for ERI=6.9, corresponding to a quite highly responding pts in terms of tumor regression.
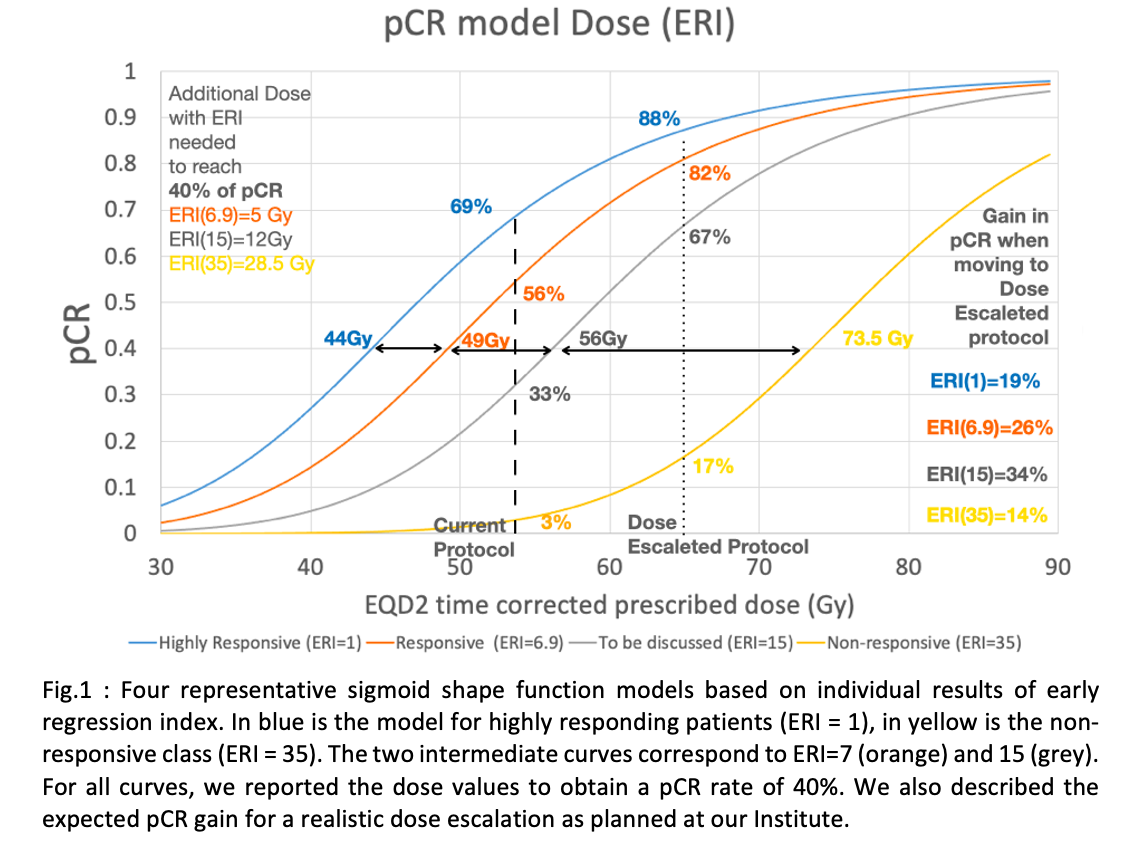
In Fig.1, we plotted four arbitrary levels of responsive pts, according to ERI values, from 1 to 35. As an example, numbers at the arrows border represent the dose corresponding to a 40% rate of pCR. The % values on the dashed and dotted lines represent the expected improvement from our current protocol (EQD2=54 Gy) to the dose planned to be delivered in a new dose escaleted protocol, delivering EQD2=65.3 Gy to the residual tumor, assessed at half-therapy. For pts with favorable ERI values, high pCR rates are expected (between 67% and 88% for ERI ranging between 15 and 1). On the other hand, the gain remains limited for poorly responding pts: for pts with ERI=35, doses >80-85Gy should be delivered to reach similar pCR rates of responding pts.
Conclusion
The suggested Logit model incorporating the individual response to RCT for rectal cancer, based on early regression, should be considered as a promising tool for therapy personalization both in identifying pts as candidates to avoid surgery and in better defining the best treatment intensification approach aimed to increase pCR substantially.