Predicting bilateral involvement in head & neck cancer using an interpretable probabilistic model
Roman Ludwig,
Switzerland
MO-0877
Abstract
Predicting bilateral involvement in head & neck cancer using an interpretable probabilistic model
Authors: Roman Ludwig1, Bertrand Pouymayou1, Jean-Marc Hoffmann1, Panagiotis Balermpas1, Jan Unkelbach1
1University Hospital Zurich, Radiation Oncology, Zurich, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
In current clinical practice, the elective clinical target volume (CTV-N) for oropharyngeal head & neck squamous cell carcinoma (OHNSCC) is defined using prevalence-based guidelines [1], which recommend extensive bilateral neck irradiation for most patients. However, the actual patient-specific risk of harboring microscopic metastases in the contralateral neck remains insufficiently quantified. We propose a probabilistic and interpretable model for predicting the personalized risk of involvement in lymph node levels (LNLs) of both sides of the neck depending on T-stage, location of macroscopic metastases, and the primary tumor’s lateralization. This may identify additional patients in whom contralateral neck irradiation can be avoided or reduced, possibly reducing toxicity.
Material and Methods
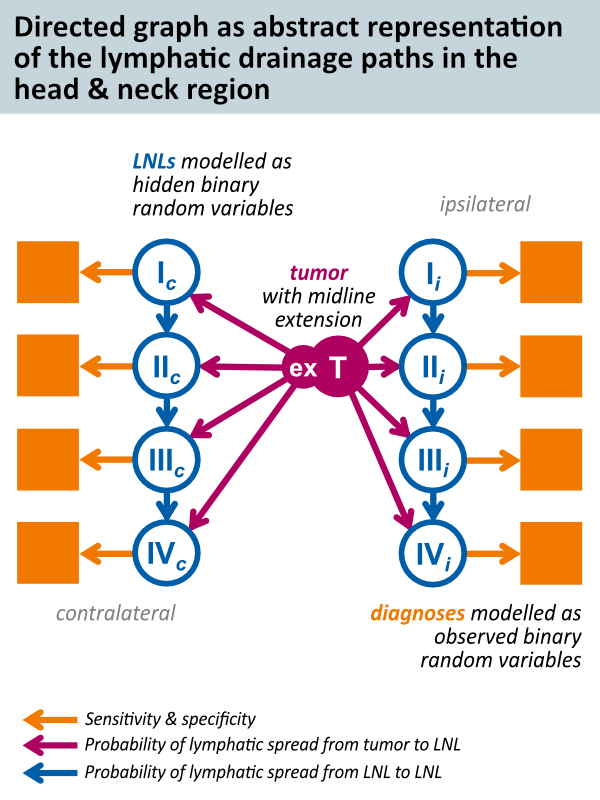
We extracted the lymphatic patterns of progression for 287 OHNSCC patients treated at our institution. The data can be visualized at www.lyprox.org. This was used to train the hidden Markov model (HMM) for predicting nodal involvement we developed and published recently [2]. For this work, the model in [2] was extended to contralateral spread while treating mid-sagittal plane extension of the primary tumor as risk factor. It models the LNLs as binary random variables connected in a directed graph (Figure 1). The edges of the graph represent the lymphatic drainage pathways, which are associated with probabilities of metastatic spread per abstract time step. These are the parameters of the HMM that are learned from the dataset of 287 patients.
Results
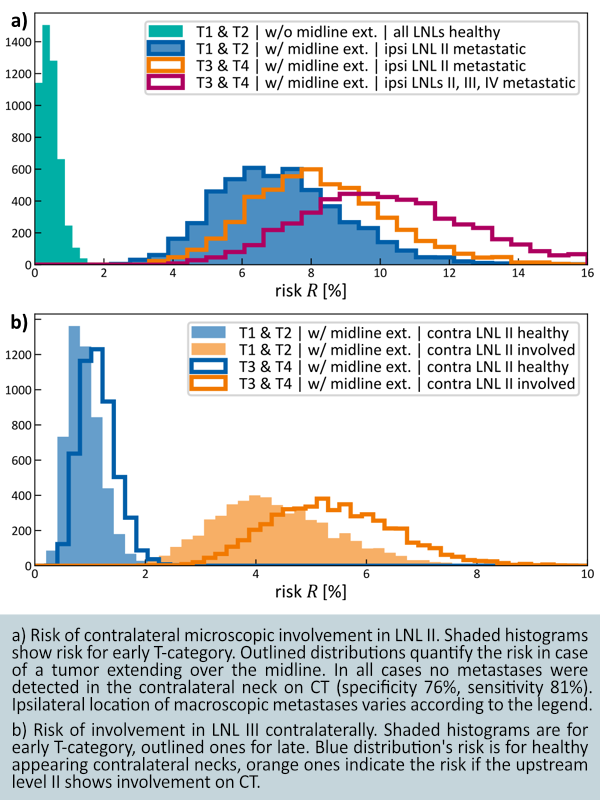
Figure 2a) shows the predicted risk of microscopic metastases in contralateral LNL II depending on T-category, the extent of CT-observed macroscopic metastases, and midline extension as a risk factor. This risk is low (0.5 ± 0.3 %) for patients with early T-category (T1 & T2) tumors not extending over the midline with no clinically involved LNLs. However, it is significantly higher when the tumor is not lateralized, and we observe ipsilateral LNL II to be metastatic (7.2 ± 1.9 %). It further increases for late T-category (8.3 ± 2 %) and once more when the ipsilateral LNLs II, III and IV are clinically involved (10.3 ± 2.6 %). Figure 2b) shows the risk predicted for involvement in contralateral LNL III depending on the upstream level II.
Conclusion
An HMM as probabilistic framework proves to be both flexible to expand and suitable for predicting the risk of microscopic involvement in a personalized manner. We can specify a patient by T-category, observed macroscopic involvement and the primary tumor’s midline extension to compute their risk for harboring microscopic metastases in any LNL recorded in the training cohort. Multi-institutional detailed datasets are however needed to validate the model’s accuracy.
References:
[1] Biau (2019) Radiotherapy & Oncology 134 1-9
[2] Ludwig (2021) Scientific Reports 11 12261