Motion management in liver SBRT and its impact on treatment time
Nicholas Hardcastle,
Australia
MO-0471
Abstract
Motion management in liver SBRT and its impact on treatment time
Authors: Nick Hardcastle1, Mathieu Gaudreault1, Adam Yeo1, Elena Ungureanu1, Rebecca Barnes2, Cathy Markham2, Sarat Chander3, Julie Chu3
1Peter MacCallum Cancer Centre, Physical Sciences, Melbourne, Australia; 2Peter MacCallum Cancer Centre, Radiation Therapy, Melbourne, Australia; 3Peter MacCallum Cancer Centre, Department of Radiation Oncology, Melbourne, Australia
Show Affiliations
Hide Affiliations
Purpose or Objective
Reduction
of respiratory motion is critical in liver stereotactic body radiotherapy (SBRT) to reduce
organ at risk dose, facilitating increased tumour dose and resultant local
control. In our institution we assess all liver SBRT patients prior to
simulation to determine appropriate motion management (MM). This retrospective
review aims to evaluate the patterns of use of MM techniques and their impact
on treatment time.
Material and Methods
For
each patient we assess suitability, in order of priority, of voluntary exhale
breath hold (EBH), free breathing gating, abdominal compression (AC), or free
breathing (FB), according to the flowchart in Figure 1. We use an external
surrogate to assess breath hold capability, followed by anterior-posterior
fluoroscopy to assess liver dome position consistency. From MM assessment
session records, we extracted liver dome position consistency in repeat EBHs,
liver dome motion change with AC and decision of MM used for simulation and
treatment. All patients were treated on a TrueBeam linear accelerator with
flattening-filter free photon beams using arc (VMAT) or static gantry (3DCRT,
IMRT) techniques, with between 6 and 20 Gy per fraction. CBCT image guidance
was used in all cases, with acquisition matched to the MM technique (free
breathing, gated or breath hold CBCT). From the record and verify system we
extracted treatment time, defined as time from first setup image to last
treatment beam off. Treatment time was assessed as a function of MM, technique
and number of CBCTs.
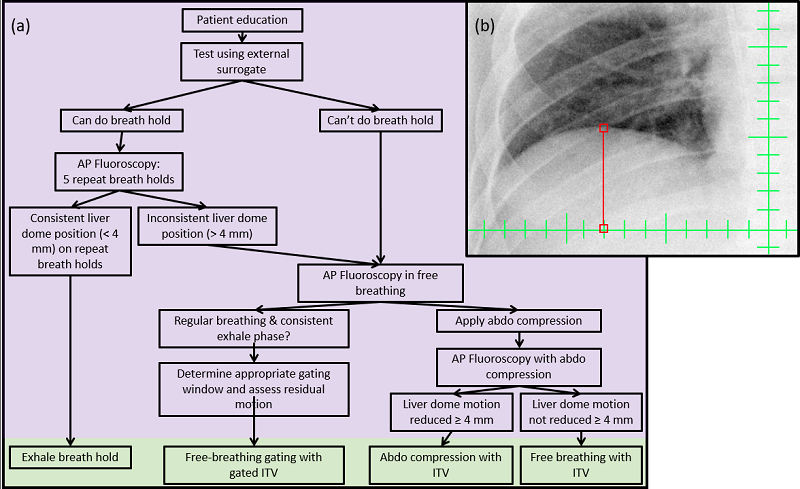
Figure 1:
(a) Workflow for assessment of appropriate MM and (b) example ant-post fluoroscopy liver
dome position
Results
From
September 2017 to September 2021, 145 patients underwent MM assessment. Of
these, 67.6% were suitable for EBH, 20.0% for AC, 6.9% for gating and 5.5% FB. 88/100
patients assessed with fluoroscopy for liver dome consistency in EBH could
achieve repeat EBH with <4mm variation. Reduction in liver motion with
AC compared with FB was highly variable (mean 3.5 mm, range -0.3-16 mm). Treatment time was available
for 613 fractions (Figure 2) and was largest for EBH (40 ± 14 min) and gated
treatments (46 ± 19 min), compared with AC (32 ± 11 min, p<0.001) and FB (27
± 12 min, p<0.001). Treatment time was independent of fraction size. Four
patients originally assessed as suitable for EBH could not achieve reproducible
EBH at treatment and were treated in FB (3) or with AC (1). Arc treatments were
quicker than static gantry treatments (35 ± 14 min vs 43 ± 15 min, p = <0.001).
Average treatment time was increased by 7 mins with each CBCT acquired.
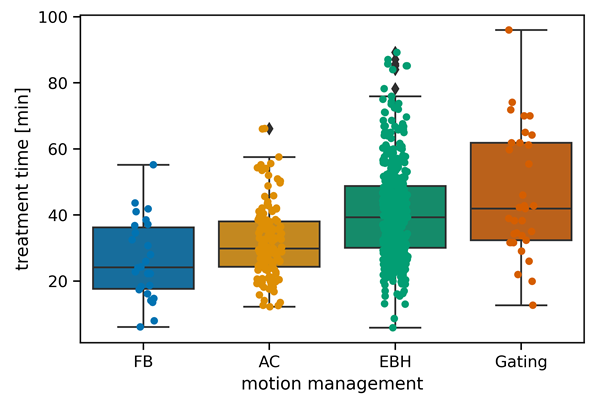
Figure 2:
Treatment time per fraction as a function of motion management approach
Conclusion
MM
in liver SBRT must be assessed per-patient to determine the most appropriate
technique for that patient. Extended treatment times must be taken into account
when deciding on optimal MM strategy. Methods to reduce intra-fraction
volumetric imaging, such as real-time imaging or tracking, may be beneficial to
reduce treatment time.