4pi-IMRT based path-finding for dynamic trajectory radiotherapy
Paul-Henry Mackeprang,
Switzerland
MO-0544
Abstract
4pi-IMRT based path-finding for dynamic trajectory radiotherapy
Authors: Paul-Henry Mackeprang1, Jenny Bertholet1, Silvan Mueller1, Gian Guyer1, Hannes A. Loebner1, Daniel Frei1, Werner Volken1, Olgun Elicin1, Daniel M. Aebersold1, Michael K. Fix1, Peter Manser1
1Inselspital, Bern University Hospital and University of Bern, Division of Medical Radiation Physics and Department of Radiation Oncology, Bern, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
Dynamic
trajectory radiotherapy (DTRT) adds dynamic table and collimator rotation during
beam-on to state-of-the-art volumetric modulated arc therapy (VMAT). While
investigations showed dosimetric benefits of DTRT plans, plan quality depends
strongly on the path-finding approach, which in our group is based on geometric
overlap between planning target volumes (PTVs) and organs at risk (OARs). In
this work, a novel path generation method was developed, which is based on
4pi-IMRT and enables automated path-finding.
Material and Methods
To
assess 4pi-based DTRT path-finding, seven common HN cancer cases on an
anthropomorphic phantom that had previously been planned with geometry based
path-finding were used. Six cases were prescribed 66-70 Gy in fractions of 2 Gy
each over 1-3 sequential phases and one case (single vocal cord irradiation,
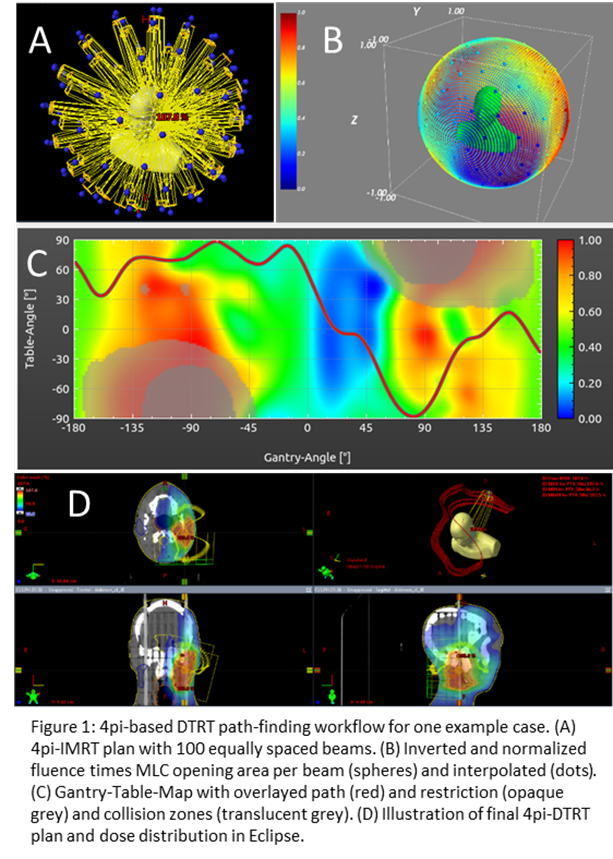
SVCI) was prescribed 58.08 Gy in 16 fractions of 3.63 Gy each. 4pi plans were generated in a
research version of the Eclipse treatment planning system v.15.6 (Varian
Medical Systems, Inc., Palo Alto, CA) with 100 equally distributed beams, and
intensity modulation was optimized using objectives from treatment planning for
geometry based DTRT (Figure 1A). From the resulting plans, the fluence multiplied
by the MLC opening area per IMRT beam was used to generate gantry-table maps
(Figure 1B and C). Like in geometry based path-finding, paths were then determined
by an A* search algorithm on these maps, excluding restriction and collision
zones (Figure 1C). The resulting paths were used to optimize DTRT plans (4pi-DTRT)
in Eclipse, again using the same objectives (Figure 1D). The 4pi-DTRT plans
were compared to geometry based DTRT plans.
Results
PTV D95% for
4pi-DTRT and geometry based DTRT plans was within +/-1%. For three
oropharyngeal cancer cases and one adenoid-cystic
carcinoma of the parotid,
mean doses to the contralateral salivary glands, pharynx and oral cavity were similar
(+/- 0.8 Gy) for 4pi-DTRT and geometry based DTRT. For a nasopharyngeal
carcinoma case, D0.03 cc to the chiasm was 1.4 Gy higher for 4pi-DTRT and contralateral
eye D0.03 cc was 1.2 Gy lower with all other relevant endpoints including
dose to the optic nerves similar (+/- 0.8 Gy). For laryngeal
carcinoma, all relevant endpoints were similar (+/- 0.8 Gy). For the SVCI
case, max dose to the spinal cord, brachial plexus, carotid arteries and mean
dose to the inferior constrictor were higher for 4pi‑DTRT by 1.3 to 2.2 Gy
and mean dose to the supraglottic larynx (-1.7 Gy) and upper esophagus (‑3.0 Gy)
were lower for 4pi‑DTRT. Mean doses to the contralateral vocal cord, arytenoid,
mid constrictor and thyroid were similar (+/- 0.8 Gy).
Conclusion
The
developed novel 4pi-DTRT path-finding is an alternative to geometry based
path-finding for DTRT treatment planning, resulting in similar plan quality for
common HN cases. It has the potential, however, of increased efficiency through
automation. This
work was supported by Varian Medical Systems, Inc.