CCI and TNM stage do not influence early mortality risk after definitive radiotherapy in NSCLC
Kristian Hastoft Jensen,
Denmark
MO-0390
Abstract
CCI and TNM stage do not influence early mortality risk after definitive radiotherapy in NSCLC
Authors: Kristian Hastoft Jensen1, Jeppe Friborg1, Ivan Richter Vogelius1, Mette Pøhl1, Malene Støchkel Frank2, Olfred Hansen3, Tine Schytte3, Charlotte Kristiansen4, Marianne Knap5, Maria Skovborg6, Tine McCulloch6, Gitte Persson7
1Rigshospitalet, Department of Oncology, Copenhagen, Denmark; 2Zealand University Hospital, Næstved , Department of Oncology, Næstved, Denmark; 3Odense University Hospital, Department of Oncology, Odense, Denmark; 4Vejle Hospital, Department of Oncology, Vejle, Denmark; 5Aarhus University Hospital, Department of Experimental Clinical Oncology, Aarhus, Denmark; 6Aalborg University Hospital, Department of Oncology, Aalborg, Denmark; 7Herlev Hospital, Department of Oncology, Herlev, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
In
patients with locally advanced non-small-cell lung cancer (NSCLC), definitive
radiotherapy (RT) or chemoradiotherapy (CRT) is associated with considerable
toxicity and approximately half of patients die within two years. A better
understanding of early mortality is needed to improve patient selection and
guide supportive interventions. In this population-based study, we investigated the
impact of the Charlson Comorbidity Index (CCI), TNM stage and performance
status on early mortality risk. We also hypothesized that there would be a
high-risk interval for early mortality, and therefore assessed the temporal
distribution of early deaths.
Material and Methods
Patients
with stages IIa, IIb, IIIa and IIIb NSCLC (according to the 7th edition of the AJCC/UICC TNM Classification) treated with RT/CRT in Denmark 2010–2017 were
included. Patients were identified in local, electronic radiotherapy charts and
additional data were obtained from the Danish Lung Cancer Registry. Patients
were excluded if the treatment was pre- or postoperative or if they received
stereotactic body radiation therapy. Early mortality was defined as death within 180
days from RT/CRT initiation. Possible risk factors, including age, sex, performance
status, TNM stage, the CCI, histology and treatment period, were investigated
using multiple logistic regression.
Results
We
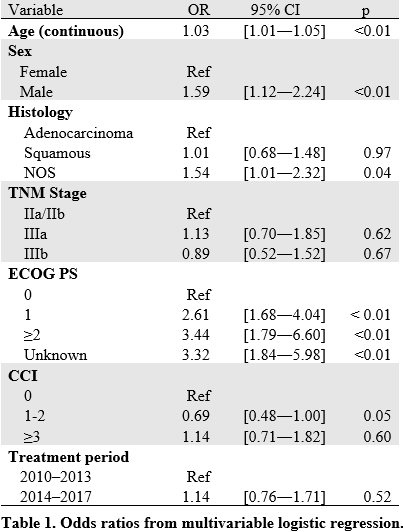
included 1742 patients and early mortality occurred in 10%. In multivariable analysis, age, sex, performance
status and tumor histology were significantly associated with the risk of early mortality, while the
CCI, TNM stage and treatment period were not (Table 1). Only a small proportion of deaths
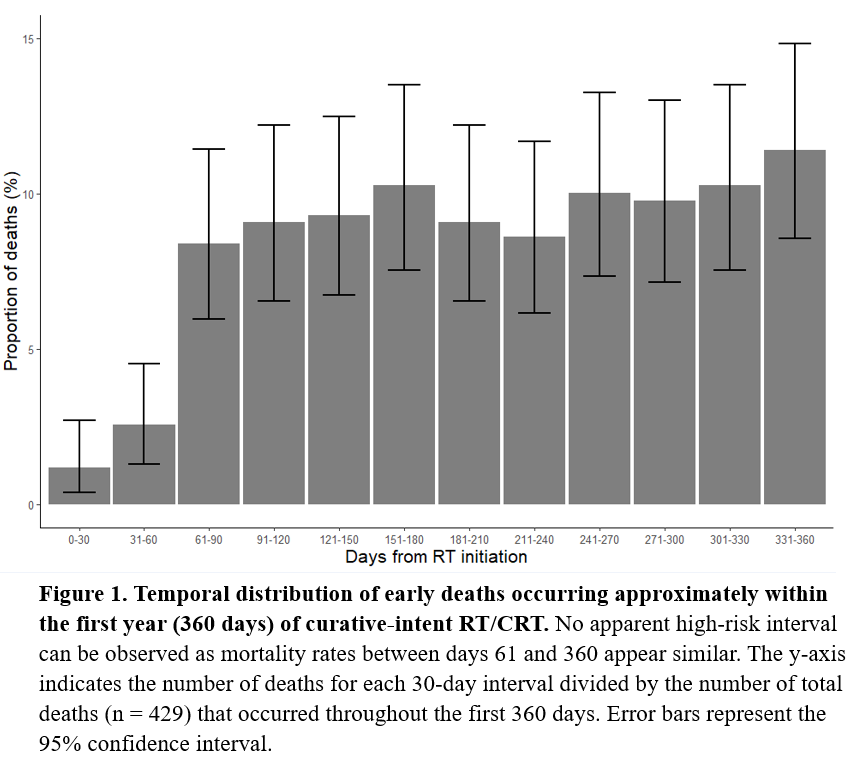
occurred during the first two months, but otherwise there was an even temporal
distribution of deaths across the first year following RT/CRT (Figure 1). Despite similar early mortality rates, patients treated between 2014-2017 had improved overall survival compared with patients treated between 2010-2013.
Conclusion
There was no discernible high-risk period
for early mortality and neither the CCI nor TNM stage was associated with an
increased risk. To optimize risk stratification, other tools than the CCI
should be used to quantify comorbidity in this setting.