Inter-observer variation in a national lung SABR rollout program: Lessons learnt & future directions
Patricia Diez,
United Kingdom
MO-0392
Abstract
Inter-observer variation in a national lung SABR rollout program: Lessons learnt & future directions
Authors: Patricia Diez1, Fiona McDonald2, Chloe Brooks1, Anoop Haridass3, Matthew Hatton4, Clive Peedell5, Yat Man Tsang6, John Conibear7
1National Radiotherapy Trials Quality Assurance Group, Mount Vernon Cancer Centre, Radiotherapy Physics, Northwood, United Kingdom; 2The Royal Marsden NHS Foundation Trust, Lung Unit, London, United Kingdom; 3Clatterbridge Cancer Centre, Department of Clinical Oncology, Liverpool, United Kingdom; 4Weston Park Hospital, Department of Clinical Oncology, Sheffield, United Kingdom; 5South Tees NHS Foundation Trust, Department of Clinical Oncology, Middlesbrough, United Kingdom; 6National Radiotherapy Trials Quality Assurance Group, Mount Vernon Cancer Centre, Radiotherapy Department, Northwood, United Kingdom; 7Barts Cancer Centre, Radiotherapy Department, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
A radiotherapy quality assurance (QA) program
was developed as part of a national plan for the expansion of lung stereotactic
ablative body radiotherapy (SABR) services. The aim was to ensure consistent,
high-quality SABR was implemented across all centres introducing this technique.
As part of the QA program, radiation oncologists’ ability to delineate
target volumes and associated organs at risk (OARs), according to UK SABR
Consortium Guidelines and Global Harmonization Group Consensus Guidelines (Mir
et al, 2020), was assessed.
Material and Methods
A
contouring benchmark case was circulated amongst 24 centres starting their lung SABR program. The 4DCT dataset sent
contained 12 individual phases. A diagnostic PET-CT was also provided. Two
clinicians from each hospital were invited to contour the ITV, PTV and 10
OARs following supplied guidance. All submissions were reviewed by a team of SABR
experts comprising 5 radiation oncologists, a medical physicist and a clinical
research fellow. Detailed feedback was provided through standardised written and
pictorial reports and any unacceptable contours were asked to be resubmitted
after further guidance from experienced mentors assigned through the implementation
program.
Consensus
volumes were agreed by all reviewers. Acceptability criteria were defined for
each structure based on cranio-caudal borders, axial under or over-contouring and
inclusion/exclusion of anatomical features as detailed in the instructions.
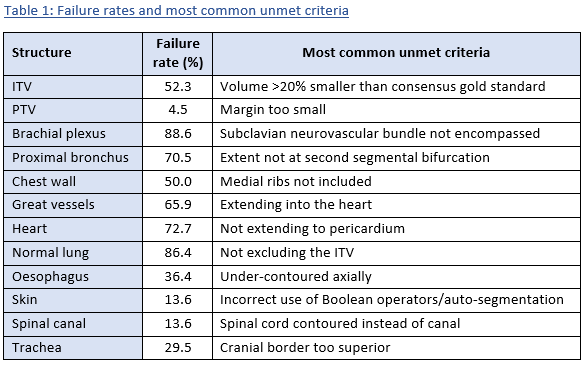
Results
44 radiation oncologists completed the benchmark
case, only one was approved on the first attempt. Failed submissions had a
median of 6 unacceptable structures (range 2-9). 52.3% of ITVs were found to be
unacceptable, mostly due to under-contouring, however most PTVs (95.5%) had
been grown correctly. 6/10 OARs had failure rates ≥50%, the brachial plexus
being the most complex structure to contour. Failure rates and the most common
reasons for structures being unacceptable are detailed in Table 1.
40/43 resubmissions were approved, with those still
unacceptable being referred to one of the 5 radiation oncologist SABR experts for
further training.
Conclusion
The outlining benchmark case has highlighted
training needs in delineation and interpretation of guidelines. Visual aids may
prove useful in future guidance. Detailed feedback was provided to aid with
education and ongoing support from mentors is in place. Contouring workshops
have also been developed and participation in peer review and clinical trials
is recommended going forward.