Parotid gland volumetric change during IMRT and implications for stem cell sparing strategies
PD-0824
Abstract
Parotid gland volumetric change during IMRT and implications for stem cell sparing strategies
Authors: Megi Gjini1, Patrik Brodin2, Sadia Ahmed3, Wolfgang Tomé2, Shalom Kalnicki4, Chandan Guha2, Rafi Kabarriti2, Madhur Garg4
1Albert Einstein College of Medicine and Montefiore Medical Center, Radiation Oncology, Bronx , USA; 2Albert Einstein College of Medicine and Montefiore Medical Center, Radiation Oncology, Bronx, USA; 3Albert Einstein College of Medicine, Radiation Oncoloy, Bronx, USA; 4Montefiore Medical Center, Radiation Oncology, Bronx, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Clinical trials investigating parotid gland stem cell (PGSC) sparing have not shown added protection from radiation-induced xerostomia, and we hypothesize that this is due to not adequately accounting for changes in the anatomy and location of the PGs during treatment. Here we evaluate the change in PG volume at mid-treatment and the association between dose to the PG or PGSC region and patient-reported xerostomia based on pre- and mid-treatment computed tomography (CT) scans for patients treated with IMRT for head and neck cancer (HNC).
Material and Methods
Patients treated from 2006-2012 at our institution with prospective patient-reported xerostomia outcomes available at least 9 months following RT were included. The PG and PGSC regions were delineated and the dose was estimated from the treatment plan 3D dose distribution, on both pre- and mid-treatment CT scans. The association between radiation dose and volumetric changes at mid-treatment was assessed using linear regression. Logistic regression and logistic dose-response models were used to examine the association between dose to the PG or PGSC region and the risk of patient-reported xerostomia.
Results
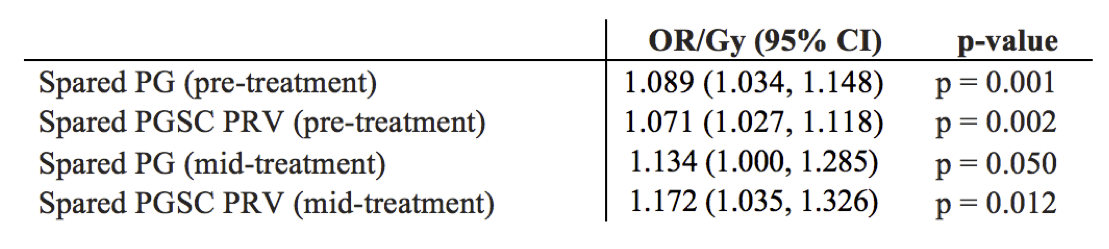
Sixty-three patients were included, most treated with 70 Gy in 33 fractions; 34 of them had mid-treatment CT scans. Figure 1 shows that both the left and right PGs had a significant volume reduction from baseline to mid-treatment (p<0.001), and that change in PG volume was significantly associated with mean PG dose (p<0.01). The logistic regression models in Table 1 show a strong association between xerostomia and radiation dose to the spared (contralateral) PG and spared PGSC region (p=0.001 and p=0.002, respectively), when assessed based on pre-treatment contours. Using the dose delivered by the time of mid-treatment CT and the adapted mid-treatment contours revealed a larger OR/Gy of 1.13 (p=0.050) for the whole PG and 1.17 (p=0.012) for the PGSC region. In line with negative results from clinical trials of PGSC sparing, our dose-response models based on pre-treatment contours estimated very similar risks of xerostomia at the 20 Gy mean dose QUANTEC-recommended constraint, with 32.5% using whole spared PG vs. 31.4% using the spared PGSC region.
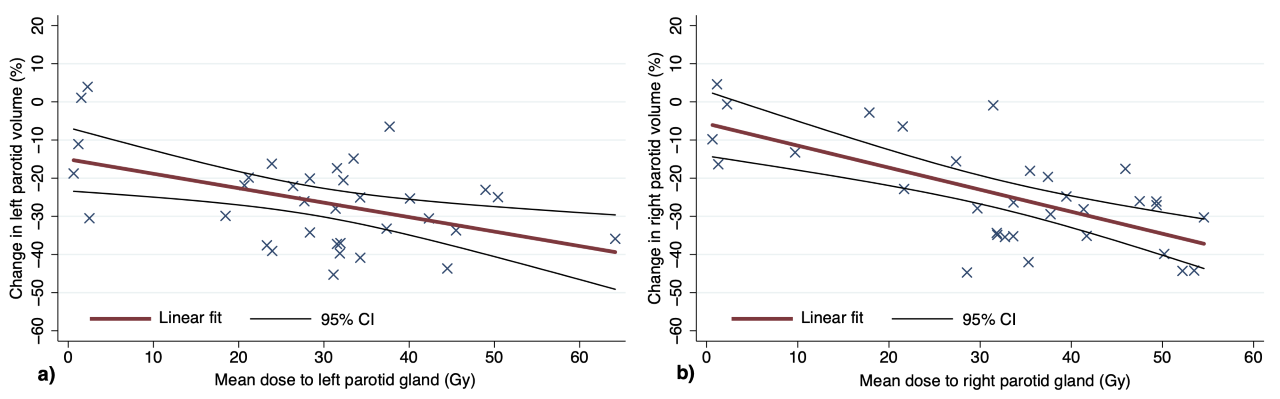 Figure 1. Linear regression showing PG volume change of left (a) and right (b).
Figure 1. Linear regression showing PG volume change of left (a) and right (b).
Table 1. Xerostomia logistic regression with dose from pre-treatment CT (n=63) or dose delivered by time of mid-treatment CT with mid-treatment contours (n=34).
Conclusion
There were significant PG volumetric changes at mid-treatment of up to 30-40% in a lot of cases, and these changes were significantly associated with mean dose to the PG. Moreover, the dose to the PG or PGSC region at mid-treatment was strongly associated with patient-reported xerostomia. These findings strongly encourage the use of adaptive planning strategies to implement more robust functional avoidance of the PGSC region during treatment, taking into account the radiation-induced shifts and shrinkage of the glands throughout treatment.