Impact of suboptimal community dose delivery on TCP in advanced radiotherapy
Vanessa Panettieri,
Australia
MO-0048
Abstract
Impact of suboptimal community dose delivery on TCP in advanced radiotherapy
Authors: Vanessa Panettieri1,2, Paige Taylor3,4, Stephen F Kry5,4
1Alfred Health, Alfred Health Radiation Oncology, Melbourne, Australia; 2Monash University , Medical Imaging and Radiation Sciences, Clayton, Australia; 3Imaging and Radiation Oncology Core, Imaging and Radiation Oncology Core, Houston, USA; 4MD Anderson Cancer Center, Radiation Physics, Houston, USA; 5Imaging and Radiation Oncology Core, Imaging and Radiation Oncology Core, Houston, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
The Imaging and Radiation Oncology Core provides end-to-end
phantom audits for institutional credentialing for clinical trials. These
indicate how well an institution can deliver their intended treatment. However,
assessment of institutional performance, and pass/fail criteria, are based on
dosimetric metrics rather than clinical acceptability. It is unclear what the
performance on this phantom, or the phantom criteria, correspond to in terms of
expected patient outcome. Therefore, we used TCP modelling to estimate clinical
outcomes associated with actual phantom deliveries in the community.
Material and Methods
A total of 322 irradiations of the IROC H&N phantom were
conducted between 2017 and 2019 by different radiotherapy centres. For each
irradiation absolute doses to 6 TLD, centrally located within the CTV, were
measured. These 6 values were used to generate CTV dDVH. Variation
of outcome as a result of dose variation was determined with the Marsden TCP
model (1)(BioSuiteVn12). The “ideal” outcome was obtained by assigning 100% of the prescribed
dose to the CTV. Model parameters were derived from the literature and the
value of sa was
adjusted to fit the model with published clinical data in terms of local
control. Because this phantom is used to credential for
all anatomical sites where IMRT is the focus, TCP modelling for three sites was done: prostate, H&N and lung. For lung, because there was substantial
difference between the standard and adjusted models, both were evaluated.
Parameters were: Intact prostate:a=0.185(1/Gy) sa=0.053, a/b=3 Gy; H&N:a=0.3(1/Gy) sa=0.09, a/b=10 Gy;
lung:a=0.307(1/Gy) sa=0.037 standard-0.080 adjusted, a/b=10 Gy, rc=1.0e7(per cc) for all sites. TCP
results were sorted based on phantom result: good(95%-105% dose agreement between
predicted and delivered in the CTV), poor(93-95% and 105-107%) and fail(<
93%, >107%).
Results
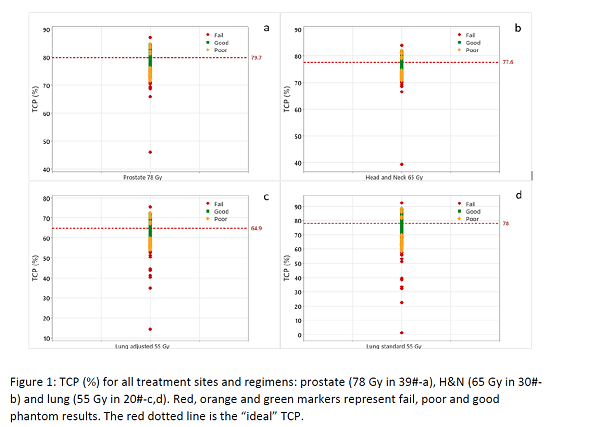
Of
the 322 phantom results, 13 failed, 38 were poor and 271 were good (Fig1). For
prostate and H&N, median TCPs were 78.4% and 76.5% respectively. TCP
decreased by 3% for poor phantom results, and by a further 5% for failing
phantoms (with TCP values as low as 46.1%(prostate) and 40%(H&N));
differences were all significant (One-way ANOVA p<0.001). For the lung, median
TCPs were 74.8% with the published and 62.9% for the adjusted parameters. TCP dropped substantially when the delivered plan did not match the
predicted plan; poor results were 8%-4% lower and failing results were a
further 20%-10% lower, with TCP values as low as 1.3% and 14.4% for standard
and adjusted respectively.
Conclusion
The variability in phantom results indicate a substantial
impact on patient outcome. In particular, failing phantom results predicted a
dramatically poorer expected tumour control. As these results are based on clinical
audit results, this work highlights a dramatic need for continual improvement
in radiation oncology.
(1)
Nahum AE, Uzan J (Radio)biological optimization of
external-beam radiotherapy. Comput Math Methods Med 2012;2012:329214