Dosimetry & toxicity comparison between CBCT-Guided and MR-Guided Prostate Ultra-hypofractionated RT
OC-0952
Abstract
Dosimetry & toxicity comparison between CBCT-Guided and MR-Guided Prostate Ultra-hypofractionated RT
Authors: Vickie Kong1, Jerusha Padayachee1, Jennifer Dang1, Winnie Li1, Victor Malkov1, Jeff Winter1, Inmaculada Navarro1, Alejandro Berlin1, Joelle Helou1, Srinivas Raman1, Peter Chung1
1Princess Margaret Cancer Centre, Radiation Medicine Program, Toronto, Canada
Show Affiliations
Hide Affiliations
Purpose or Objective
Ultra-hypofractionated (³6Gy/fraction) radiotherapy for
localized prostate cancer has been delivered at our institution with either online
CBCT-guided 3 degrees of freedom (3DOF) translational correction or online MR-guided
adaptation. Herein, we compared the daily dosimetry and acute toxicity between
these two systems.
Material and Methods
Fifty patients recruited to a Phase
2 trial evaluating the efficacy of External Beam Radiation Therapy (EBRT) plus High
Dose Rate Brachytherapy intraprostatic boost (1500cGy/1) were included in this
analysis. Hydrogel spacer was inserted at the discretion of physicians. An EBRT
reference plan was generated to deliver 3000cGy/5 to the CTV (Prostate ± Seminal Vesicles) with a margin of 5mm using VMAT for 25 patients
treated with CBCT-3DOF. The remainder were planned with IMRT and MR-guided
adapt-to-shape (AtS). Daily EBRT delivered dose to CTV, bladder and rectum was computed
using the daily CBCT or MR images. Deviation of >10% from reference dose was
considered clinically significant. Acute toxicity was prospectively recorded
using Common Terminology Criteria for Adverse Events (ver 4.0).
Results
Delivered dose per fraction to 95%
of CTV was acceptable for all 250 fractions, with a median of 660cGy (Range: 649–680cGy).
Hydrogel spacer was present in 17 patients in the CBCT-3DOF and 15 patients in
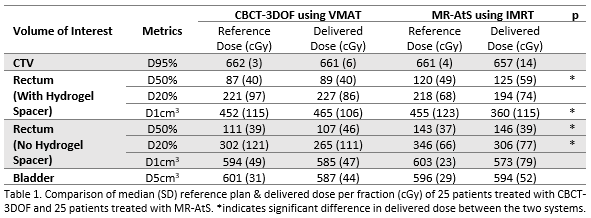
the MRL cohort. VMAT with CBCT-3DOF was associated with lower daily rectal D50%
but higher D1cm3 compared to IMRT using MR-AtS, especially in the
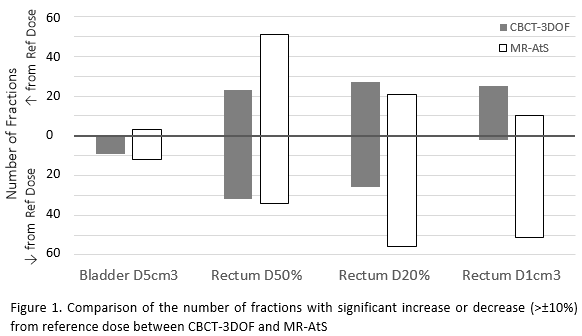
presence of hydrogel spacer (Table 1). The use of MR-AtS resulted in more
fractions delivering a significantly lower rectal D20% and D1cm3
than the reference dose, when compared to CBCT-3DOF (56 vs 26 for D20%, 51 vs 2
for D1cm3; Figure 1). In contrary, difference between reference and delivered
dose to 5cm3 of bladder was significant in <15 fractions by
either systems. Median follow up was 26 months for CBCT-3DOF and 25 months for
MR-AtS. The cumulative incidence of G2+ urinary/gastrointestinal toxicity by 6
months was 8%/8% for the CBCT-3DOF cohort and 20%/0% for the MR-AtS.
Conclusion
Significant deviation from the reference plan
dose for rectum was observed with both systems due to large range of anatomical
changes exhibited between planning and treatment sessions. MR-guided adaptation
was able to deliver a lower than reference plan dose to the rectum in the high
dose region more frequently than CBCT-guided 3DOF, and these patients
experienced a lower incidence of G2+ GI acute toxicity. Follow up is ongoing and
will assess the clinical efficacy of these two treatment delivery systems.