heart sparing in treatment planning for esophageal cancer VMAT: at what cost for lung dose?
Marijke de Boer,
The Netherlands
OC-0951
Abstract
heart sparing in treatment planning for esophageal cancer VMAT: at what cost for lung dose?
Authors: Marijke de Boer1, Antoinette Arents-Huls1, Roel G. J. Kierkels1, Paul M. Jeene1, Karin Muller1
1Radiotherapiegroep, Department of radiation oncology, Arnhem, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Traditional
treatment planning for esophageal cancer was mainly concentrated on target
coverage and lung dose reduction while accepting relatively high dose to the
heart. Recently a normal tissue complication probability (NTCP) model based
indication protocol for treatment modality selection (i.e. photon or proton
therapy) has been implemented in the Netherlands, in which a predicted 2 year
overall survival (OS) increase of 5% is required to select for proton therapy.
The NTCP model uses the volume of the GTV and the neo-adjuvant therapy status
as clinical factors. The mean heart dose (MHD) is the only dosimetric parameter
in the NCTP model. Consequently, a lower MHD directly leads to a higher
predicted overall survival. Lowering MHD leads to an increase in lung dose with
a possible increase of pulmonary toxicity. In this study, we investigated the
trade-off between heart and lung dose sparing in photon radiotherapy for
esophageal cancer patients.
Material and Methods
At least
five plans with varying heart and lung doses were optimized for seven
esophageal cancer patients treated with volumetric arc therapy in 23 or 28
fractions of 1.8 Gy (patient characteristics in table 1). While maintaining
adequate target coverage (planning target volume D95≥98%), the following plans
were created: (1) optimal lung sparing; (2) optimal heart sparing; (3) a range
of plans, each with a step-wise increase of approximately 1 Gy mean lung dose
(MLD), while lowering the MHD as much as possible. For all plans the estimated predicted
2 year overall survival was derived from the NTCP model. Also, plan robustness
was assessed by recalculation of the plan on the inhale and exhale phase of the
4DCT.
Results
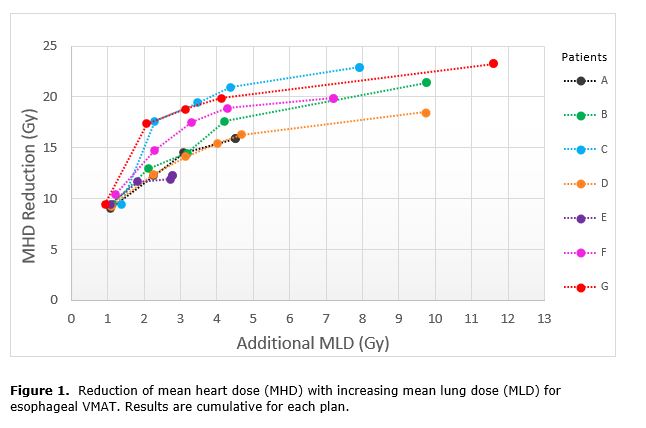
In total,
41 plans were optimized with varying lung and heart dose levels. All plans
except the maximum heart sparing plans were sufficiently robust for breathing
motion. As compared to the maximum lung sparing plan, the MHD could be reduced
by approximately 9.5 Gy for a 1 Gy increase in MLD. On average, approximately 3
Gy increase in MLD resulted in 15.8 Gy reduction of MHD. Increasing the MLD
more than 3 Gy did not lead to substantial better heart sparing in our patients
(figure 1). The mean predicted 2 year overall survival of
the maximal lung sparing plans was 38% (range 23–60%). Increasing the MLD with
approximately 3 Gy resulted in an average predicted 2 year overall survival of
49% (range 32–77%), while the predicted 2 year overall survival of the maximum
heart sparing plan was very similar: 52% (range 34–80%).
Conclusion
The mean
heart dose can be reduced substantially with only limited increase of mean lung
dose. Increasing the mean lung dose with approximately 3 Gy relative to a
maximum lung sparing esophageal VMAT plan is recommended to optimally reduce
the MHD without compromising plan robustness.