USE OF VALUE-BASED-HEALTHCARE TO EVALUATE A NOVEL TREATMENT PROTOCOL FOR LOCALIZED PROSTATE CANCER
Alfonso Gomez-Iturriaga,
Spain
OC-0923
Abstract
USE OF VALUE-BASED-HEALTHCARE TO EVALUATE A NOVEL TREATMENT PROTOCOL FOR LOCALIZED PROSTATE CANCER
Authors: Alfonso Gomez Iturriaga1, David Buchser1, Marina Marban1, Iñigo San Miguel1, Iratxe Raton1, Jon Cacicedo1, Francisco Casquero1
1Cruces University Hospital. Biocruces Bizkaia Health Research Institute, Radiation Oncology, Barakaldo, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
In 2017 the Value-Based-Healthcare (VBHC) methodology was implemented in our institution for all patients undergoing definitive treatment for prostate cancer. This methodology allows us to evaluate and compare different treatment modalities assessing prospectively patient reported (PROMS) and clinical outcomes
The objective of the present study is to compare PROMS, outcomes and costs between both treatment modalities based on VBHC-ICHOM methodology. In this analysis we will focus on quality of life outcomes.
Material and Methods
Our current standard of care for intermediate and high-risk disease prostate cancer is the combination of high-dose- rate Brachytherapy (HDR) and moderate hypofractionated Volumetric-Modulated-Arc-Therapy to a dose of 37.5Gy in 15 fractions (HDR-VMAT).
In June 2019, we launched a prospective phase II clinical trial investigating a novel radiation schedule, consisting of the combination of HDR (15Gy) and Stereotactic-Ablative-Radiotherapy to a dose of 25Gy in 5 daily fractions (HDR-SABR)
From April 2017 to August 2021, 91 consecutive patients with intermediate/high-risk have received HDR-VMAT, and between April 2019 and August 2021, 72 patients received HDR-SABR
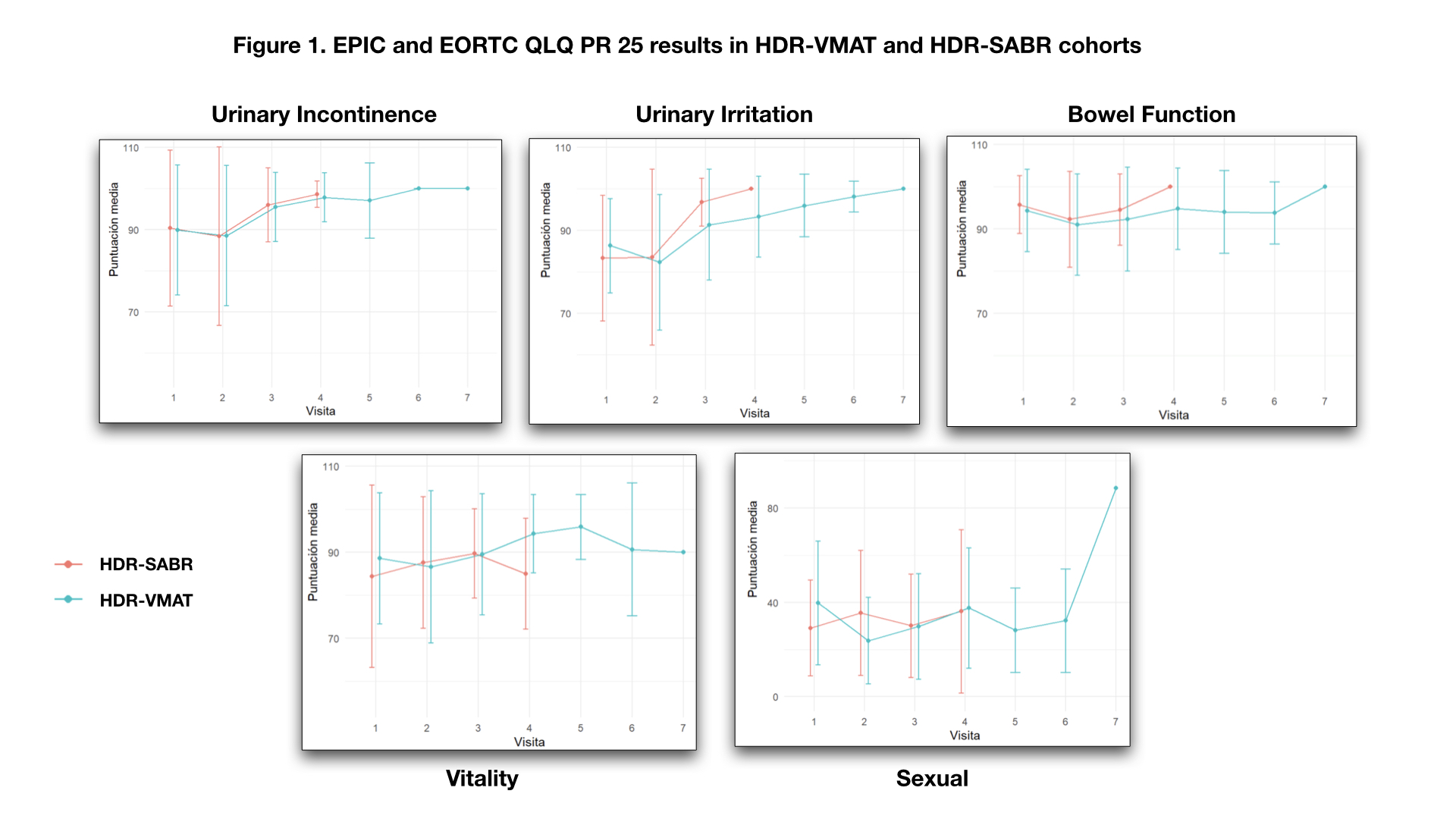
The patients were monitored prospectively for toxicity (CTCAE v. 4.0) and health-related quality of life (Expanded Prostate Cancer Index Composite [EPIC] and EORTCQLQ- PR25). A clinically significant decrement was considered an EPIC score decrease greater than one-half of the SD of the baseline value for each domain.
Results
No statistically significant differences were found in clinical and pathological characteristics between both groups. Overall, median initial PSA was 11 (range 8-19). Based on DRE, 70% of patients had cT1c tumors, 25% were T2a-T2c and 2% were T3a. After mpMRI, 63% were T2a-T2c and 30% were T3a-T3b. ISUP grade was 1 in 29%, ISUP2 in 41%, ISUP3 in 14.5% and ISUO4-5 in 15.5%.
Median prostate volume was 37cc (range 27-49.5cc) and median baseline IPSS was 4 (range 3-10)
The median follow-up for the HDR-VMAT cohort was 20 months and 12 months for the HDR-SABR cohort.
No severe (i.e. G3-4) acute or late events were recorded. Grade GU and GI grade </= 2 toxicity rates were similar between groups.
No significant decline in patient QoL (0.5 x standard deviation) between the standard and the experimental treatment was observed in any domain (Urinary incontinence, urinary irritation, bowel, vitality and sexual domains) after evaluation using ICHOM methodology.
Conclusion
The combination of HDR boost and SABR (25Gy in 5 fractions), demonstrates excellent results in terms of toxicity, tolerance, safety, patient satisfaction and impact on HRQoL. No differences were found between the experimental treatment and our standard treatment of HDR-VMAT (37.5Gy in 15 fractions). Longer follow-up is needed to confirm the efficacy of the novel strategy.