Health-economics and evidence-based hypofractionation uptake in Europe: GIRO-HERO cluster analysis
OC-0920
Abstract
Health-economics and evidence-based hypofractionation uptake in Europe: GIRO-HERO cluster analysis
Authors: Julieta Corral1, Carol Oliveira2, Ramon Clèries1, Danielle Rodin3, Josep Maria Borras4, Yolande Lievens5
1Department of Health, Generalitat de Catalunya, Catalan Cancer Plan - IDIBELL, Barcelona, Spain; 2Cancer Center of Southeastern Canada, Department of Oncology, KIngston, Canada; 3Princess Margaret Cancer Centre Toronto, Radiation Medicine Program, Toronto, Canada; 4University of Barcelona, Department of Clinical Sciences - IDIBELL, Barcelona, Spain; 5Ghent University Hospital, Department of Radiation Oncology, Ghent, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
Health-economic factors have been suggested to affect evidence-based hypofractionation uptake (HFU) in curative breast and prostate cancer, and palliative radiotherapy (RT). The study objective is to identify clusters of countries with different socio-economic and RT service-related factors and their influence on HFU in Europe.
Material and Methods
A hierarchical clustering analysis based on principal components was carried out to assess differences in the HFU in 40 European countries for curative breast (breast-conserving, node negative) and prostate cancer (low-risk), and palliative irradiation of uncomplicated bone metastases. Included variables are GNI per capita, MV units/million inhabitants, actual RT courses both as % of all incident cancer cases, and as % of optimal number of courses defined by evidence-based guidelines. Country-specific 5-year relative survival was included for breast and prostate cancer. HFU data was derived from the 2018 ESTRO-GIRO survey, while RT service-related factors were obtained from the ESTRO-HERO project. Socio-economic data were extracted from publicly available databases. Once the clusters were defined, the average of all variables within each cluster was calculated, including hypofractionation-specific reimbursement. After a sensitivity analysis, only 36 countries were included in the analysis.
Results
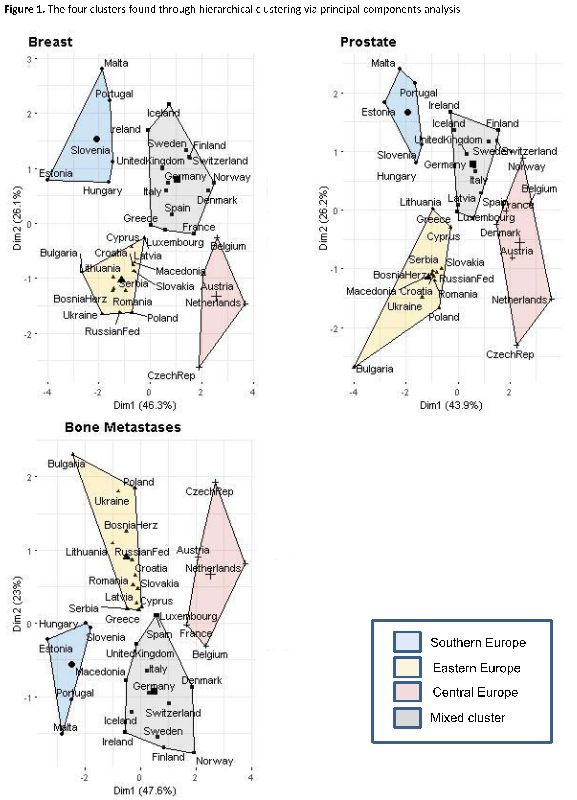
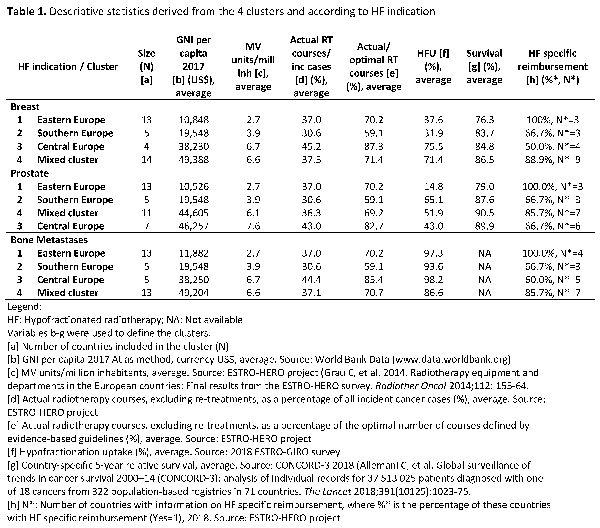
The optimal number of clusters is 4, with an Eastern European countries cluster, a Southern cluster (including Estonia and Hungary), and 2 clusters that include more Western European countries (one denoted as ‘Central Europe’ the other as ‘Mixed Cluster’) (Figure 1). The GNI per capita has an important impact in defining the clusters, with Eastern and Southern Europe clusters having lower GNI/capita values and lower number of MV units per million inhabitants compared to Western clusters (Table 1). Higher HFU is observed in Western countries compared to Eastern and Southern countries for breast cancer, while Southern countries have highest HFU for prostate cancer. Countries with the lowest average GNI per capita and RT availability underutilize HF for both curative breast and prostate cancer (Eastern European cluster). The two clusters with higher average GNI per capita (Western European clusters), both having high RT availability and survival, show a negative correlation between HFU in palliation and HF-specific reimbursement, while HFU is similar for curative intent RT, without impact of reimbursement.
Conclusion
Four clusters of European countries were identified based on their HFU and health-economic factors with a few countries being allocated differently depending on the treatment site. Cluster definition is related to GNI per capita, and ensuing RT availability, with variable impact on HFU. These insights may support national policy-makers and scientific societies in their pursuit of optimal HFU, and endorse better dissemination of this therapy across countries.