Hypofractionation and the risk of post radiation mucosal ulcers in oropharyngeal carcinoma.
Gerda Verduijn,
The Netherlands
MO-0479
Abstract
Hypofractionation and the risk of post radiation mucosal ulcers in oropharyngeal carcinoma.
Authors: Gerda Verduijn1, Steven Petit2, Nienke Sijtsema2, Iris Lauwers2, Yvette van Norden2, Aniel Sewnaik3, Remi Nout1, Aad van der Lugt4, Mischa Hoogeman1, Wilma Heemsbergen5
1Erasmus MC Cancer Institute, Radiation Oncology, Rotterdam, The Netherlands; 2Erasmus MC Cancer Institute , Radiation Oncology, Rotterdam, The Netherlands; 3Erasmus MC, Otorhinolaryngology and Head and Neck surgery, Rotterdam, The Netherlands; 4Erasmus MC , Radiology, Rotterdam, The Netherlands; 5Erasmus MC Cancer Institute, Radiation oncology, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Post radiation mucosal ulcers (PRMU) can have a huge negative impact on
quality of life in patients with oropharyngeal squamous cell carcinoma (OPSCC).
However, information on risk factors, and in particular on the impact of
hypofractionation, is scarce. Therefore, the goal of this study was to
determine the pattern of late PRMU development and to identify risk factors
after hypofractionated and conventional radiotherapy for OPSCC.
Material and Methods
We performed a retrospective cohort study in 332 consecutive OPSCC
patients with cT1-T4N0-N3M0 disease. Patients were included who survived at
least one year after treatment with curative intent between January 2009 and
June 2016. Patients were treated using: 1) conventional IMRT (70 Gy in 2 Gy fractions),
or 2) IMRT (46 Gy in 2 Gy fractions)
followed by a hypofractionated stereotactic body radiotherapy (SBRT) boost (16.5
Gy in 5.5 Gy fractions). Grade ≥ 2 PRMU (i.e. symptomatic PRMU according to
CTCAE v5.0) was scored in case one or more ulcers were observed > 3 months
after the last RT fraction. Two types of PRMU were distinguished: late PRMU
arising several months after RT and PRMU directly evolving from malignant
tissue without the evidence of remaining tumor tissue. Patient and treatment
related risk factors were analyzed with uni- and multivariable regression
analysis. In a subgroup of 25 patients imaging at time of PRMU was available.
The PRMU in these patients were delineated on the original planning CT scan and
location with respect to isodose lines was determined.
Results
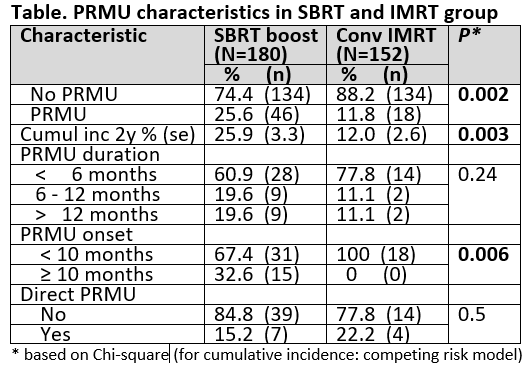
A total of 64 patients developed PRMU grade ≥ 2, with a two year
cumulative incidence of 19%. For conventional fractionation, all PRMU occurred
within 9 months (N=18). For the hypofractionation boost group (N = 46), 31 PRMU
developed within 9 months, and an additional 15 PRMU developed after 9 to 22
months post-RT (see figure). All PRMU were successfully managed (50% with HBOT),
with none developing into grade 3 PRMU. 34% of PRMU persisted after more than 6
months. The cumulative incidence of PRMU after the hypofractionation boost was
significantly higher compared to conventional fractionation (26% vs 12% at two
yrs; p = 0.003). In the hypofractionation boost group, tonsil subsite (SHR =
2.70; p = 0.003), female (SHR = 2.07; p = 0.016), and acute tube feeding (SHR =
3.10; p < 0.001) were associated with increased PRMU risk in multivariable
regression. In the conventional fractionation group, no statistically significant
risk factors were identified. 17% of PRMU (N = 11) developed directly after
tumor regression and the remaining 83% were late PRMU (see table). All 25
delineated PRMU were situated within the 95% isodose lines.

Conclusion
The increased risk of PRMU should be considered when introducing
hypofractionation in radiotherapy of oropharyngeal cancer. In this group,
requiring a feeding tube (surrogate for severe acute mucositis) and being
female was associated with increased risk.