From 2007 to 2020,
498 patients met the eligibility criteria. Before Jan 2018, 371 OPC patients
were treated with photons. From Jan 2018 to Dec 2020, 81 patients were treated
with IMPT and 46 patients with photons.
In univariate
analysis, ULCER1-year was 10.5% after photons and 10.8% after IMPT
(p=0.478). Most ulcers 47 (87%) were scored as grade 1 (no complaints) or grade
2 (conservative treatment), while 7 patients (13%) progressed into grade³3 (requiring surgery,
life-threatening or death). Median time to first occurrence was similar between
both groups: 5.0 months (IQR: 3.6 to 7.2) after photons and 5.8 months (IQR:
4.4-10.1) after IMPT. No difference was noted regarding recovery which was 4.1
months (IQR: 2.5-6.9) and 4.6 months (IQR: 2.4-7.8) after photons and IMPT,
respectively.
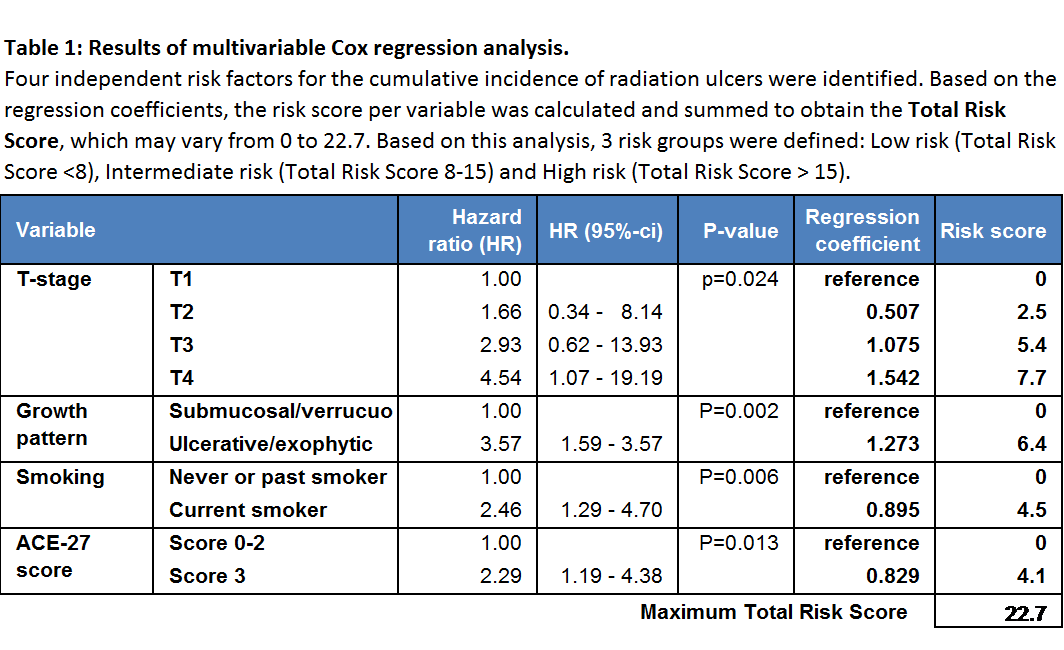
Multivariable
analysis identified 4 risk factors, including T-stage, ulcerative/exophytic
growth pattern, smoking during treatment and ACE-27 comorbidity score (Table
1). When IMPT was forced into this multivariable model, IMPT was again not associated
with an increased risk of the cumulative risk of radiation ulcer (P=0.546).
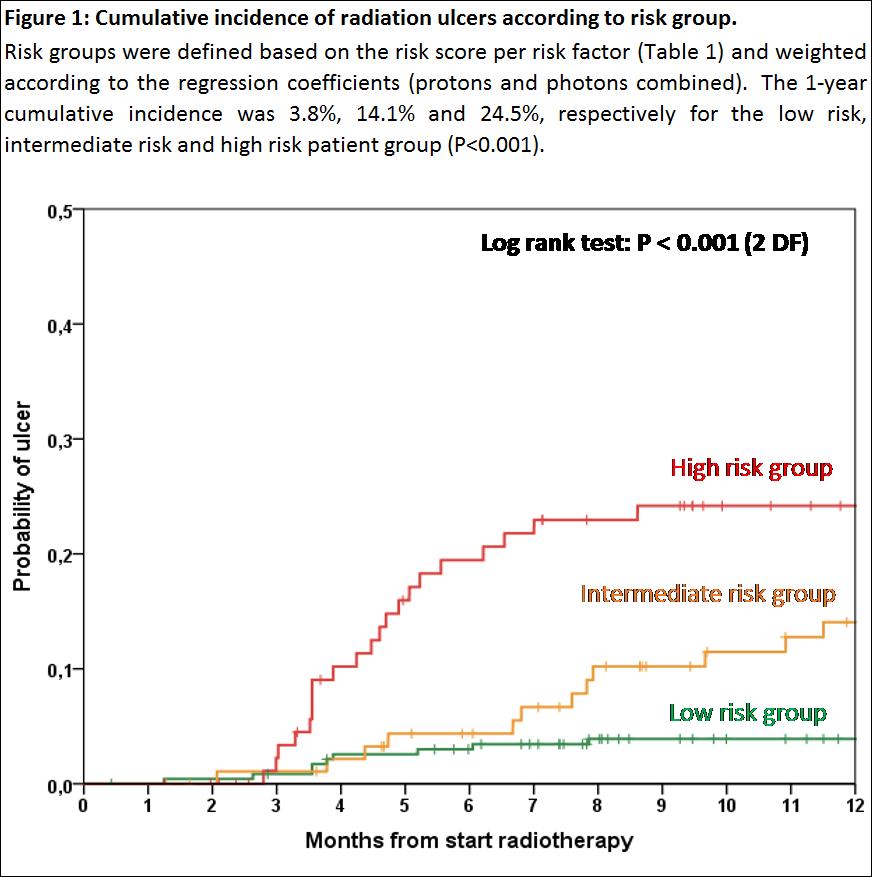
Based on the
multivariable analysis, 3 risk groups were defined (Table 1), which was a
strong predictor for the risk of ULCER1-year (Figure 1)