Risk of cardiac death increases with dose to cardiac sub structure avoidance region in lung cancer
OC-0441
Abstract
Risk of cardiac death increases with dose to cardiac sub structure avoidance region in lung cancer
Authors: Azadeh Abravan1, Corinne Faivre-Finn1, Kathryn Banfill1, Alan Mcwilliam1, Marcel van Herk1
1The University of Manchester, Division of cancer sciences, MANCHESTER, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
There is emerging evidence that radiotherapy
(RT) dose to cardiac substructures, specifically those located at the base of
the heart, is associated with cardiac events and worse overall survival in lung
cancer patients. Darby et al reported a linear relationship between excess major
cardiac events and mean heart dose in patients with breast cancer. We
investigated if a similar relationship exists for lung cancer patients treated
with curative-intent RT, considering heart substructures dose.
Material and Methods
2488 lung cancer patients treated between
2010-2016 at a single institute with radical RT (55/60-66Gy in 20/30-33
fractions) with or without chemotherapy were included. Primary endpoint was cardiac
death (CD) occurring after day 1 of RT. Cause of death recorded on death
certificates was categorised using WHO-ICD10 codes from Public Health England
data. Pre-existing cardiac disease (PCD) prior to RT was collected from
Hospital Episode Statistics data. For each patient, the planning CT scan was
deformably registered (using NiftyReg non-rigid registration) to 6 template
patients with a cardiac avoidance region (CAR) segmented by a radiation
oncologist. CAR was defined in consensus with a cardiologist based on previous
studies and included superior vena cava,
right atrium, aortic root, and proximal segments of the coronary arteries. Mean CAR dose was calculated for all patients and averaged over the 6 sets. A nested
case-control design was used, with cases being patients who died with a cardiac
cause. Each case was matched with three controls according to age range,
gender, PCD, tumor volume quartile, RT, and chemotherapy regimen. Rate ratios for
CD were estimated with the use of conditional logistic regression after
stratification. The rate of CD was modelled as bx, where x was the EQD2(α/β=3) dose to CAR (in
Gy) and b (slope) was the percentage increase in the rate CD per Gy.
Results
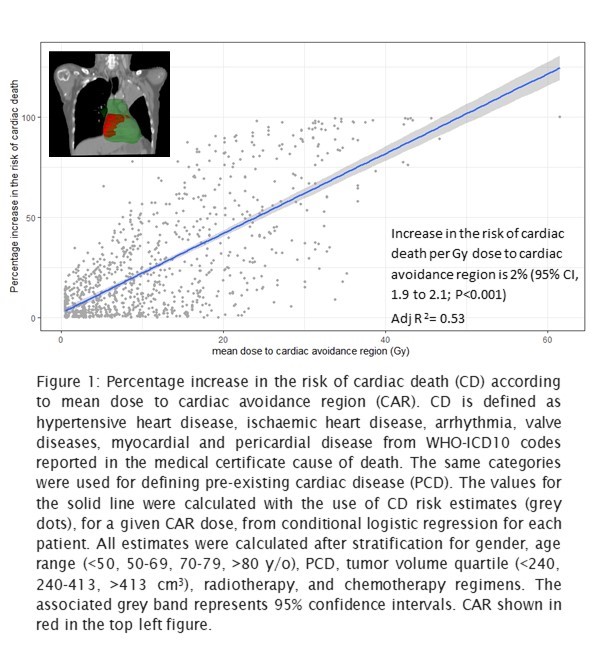
709 (28%) had PCD and 289 (12%) of the patients
died with a cardiac cause. Median of the mean
EQD2 dose to CAR was 9.9 Gy (range, 0.5-61.5) and 10.8 Gy (range, 0.5-58.7) for
patients with and without PCD, respectively. The rate of CD increased by 2% for
each 1 Gy increase in the mean radiation dose delivered to CAR (95% CI of slope,
1.9 to 2.1;p<0.001)(Fig.1). From conditional logistic regression, rate ratio
for CD among patients with PCD was similar to those without PCD (RR=1.01, 95%
CI, 0.74 to 1.36;p=0.97).
Conclusion
This study demonstrates that risk of CD increases with
mean dose to CAR, mostly located at the base of the heart, by 2% per Gy. This
study could not identify any apparent threshold for CD due to dose to CAR. The percentage
increase in the risk of CD per Gy increase in the mean CAR dose was similar for
patients with and without PCD. However, for a given dose to CAR, the absolute increase
in the risk of CD for patients with PCD will be different due to baseline risk being
different. A future study will evaluate the impact of reducing dose to CAR on lung
cancer survival in our institution.