A deformation model for the rectum which combines population and patient-specific motion patterns
OC-0942
Abstract
A deformation model for the rectum which combines population and patient-specific motion patterns
Authors: Øyvind Rørtveit1,3, Liv Bolstad Hysing1,3, Andreas Stordal2,4, Sara Pilskog1,3
1Haukeland University Hospital, Dept. of oncology and medical physics, Bergen, Norway; 2NORCE, Energy dept., Bergen, Norway; 3University of Bergen, Department of physics and technology, Bergen, Norway; 4University of Bergen, Department of mathematics, Bergen, Norway
Show Affiliations
Hide Affiliations
Purpose or Objective
The rectum, a key organ-at-risk in pelvic radiotherapy (RT), is highly deformable. Better statistical models for rectum shape changes can improve precision in RT delivery and toxicity assessment. Previous organ deformation models extract dominant motion patterns from principal component analysis (PCA). These are either patient-specific models that require several images to achieve prediction accuracy, or population models, which can describe random variations with only a single image, but lack the ability to describe individual variations accurately.
Our aim was to create a model that could combine patient-specific data and population data to achieve accurate predictions with only one or a few scans.
Material and Methods
For 37 prostate cancer patients, 8-11 CTs were taken during their RT treatment, forming a total of 371 scans. The rectum was manually contoured in all CTs, and deformable registration was used to find point-to-point correspondence of the rectal surfaces both intra-patient and inter-patient. The resulting vector fields were used as input to the model.
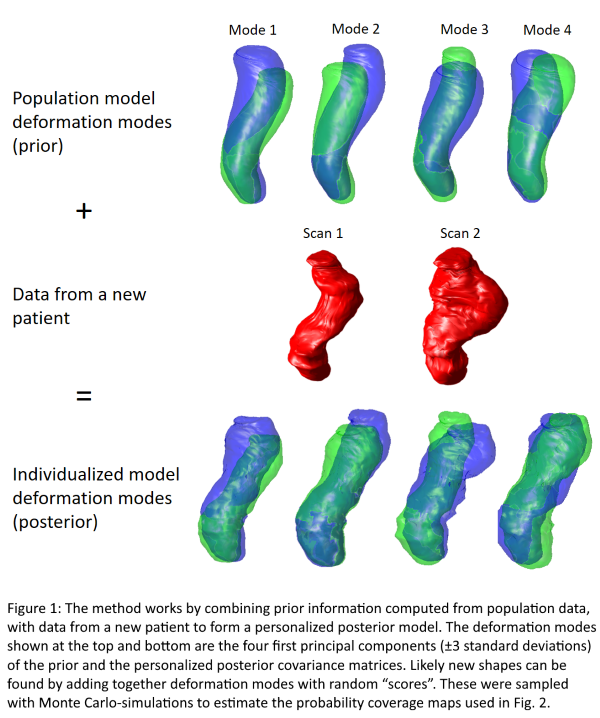
We used an empirical Bayes method where a vector p of point-coordinates on the rectum surface is modeled as multivariate normal distributed with mean vector μ and covariance matrix R. In the Bayesian context, these parameters are stochastic. We chose a practical prior distribution for the parameters; the normal-inverse-Wishart distribution. We found the hyperparameters (the parameters of the prior) by maximum likelihood estimation over the population data. When a new scan for a patient becomes available, the patient-specific parameters are updated with the corresponding vector field, creating a patient-specific posterior distribution, illustrated in Fig. 1. Because both intra-patient and inter-patient data are used in the training, the model is able to predict both random and systematic errors.
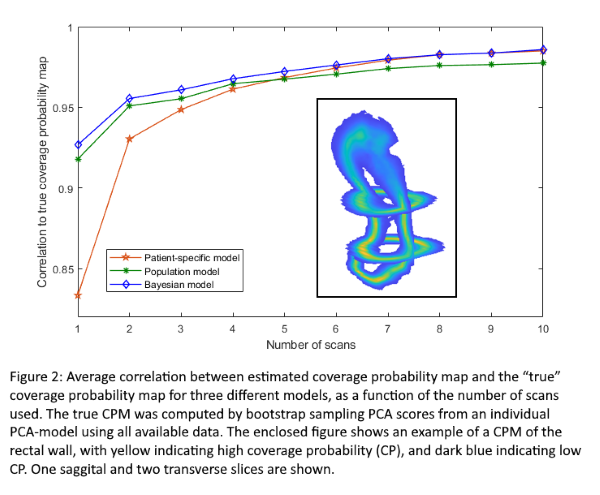
To evaluate the method, we used the deformation model to generate coverage probability maps (CPMs). These are 3D matrices of voxels, where the value in each voxel corresponds to the probability that the organ will cover that voxel at any given time (see enclosed frame in Fig. 2). We then found the spatial correlation between the estimated CPMs and the “true” CPMs, which were calculated using all patient-specific data. We evaluated the model as a function of the number of scans (1-10), and compared the Bayesian method to a pure population model and a pure patient-specific model.
Results
The results are shown in Fig. 2. The proposed method consistently outperforms the population model, while the patient-specific model converges towards the same performance as the Bayesian model given seven or more scans.
Conclusion
The new method successfully combines population data with patient-specific data to outperform both a patient-specific model and a population model. The results are also indicative of the severe limitations of patient-specific models when few scans are available.