The role of radiation therapy in the treatment of primary hepatic lymphomas
OC-0296
Abstract
The role of radiation therapy in the treatment of primary hepatic lymphomas
Authors: Jennifer Ma1, Remy Daou2, Josiane Bou Eid2, Jisun Lee1, Beatrice Fregonese1, Joe El-Khoury2, N. Ari Wijetunga1, Harper Hubbeling1, Kathryn Tringale1, Emily Lebow1, Brandon Imber1, Joachim Yahalom1, Carla Hajj1
1Memorial Sloan Kettering Cancer Center, Radiation Oncology, New York, USA; 2Saint Joseph University of Beirut, Family Medicine, Beirut, Lebanon
Show Affiliations
Hide Affiliations
Purpose or Objective
Primary
hepatic lymphomas (PHL) are an extremely rare form of non-Hodgkin Lymphoma
(NHL) for which there are no established treatment guidelines, with available
literature largely comprised of small case reports. Therefore, we evaluate
our institutional experience treating PHL within the context of existing
literature to better understand treatment modalities, role of radiotherapy
(RT), and outcomes.
Material and Methods
We conducted a single institutional retrospective
analysis of all PHL patients (pts) diagnosed from 2000-2021 with a
biopsy-proven liver lesion without other lymphomatous solid organ involvement,
except for concurrently diagnosed splenic lymphomas. Subgroup analysis was
performed for diffuse large B-cell lymphoma (DLBCL) and indolent lymphomas,
which included marginal zone (MZL), follicular (FL), and low-grade B-cell
lymphoma (BCL), NOS. Univariable (UVA) and multivariable analysis (MVA) for
overall survival (OS) was performed using the Cox proportional hazards model. A
literature review was conducted using key words “liver”, “lymphoma”, and
“treatment.”
Results
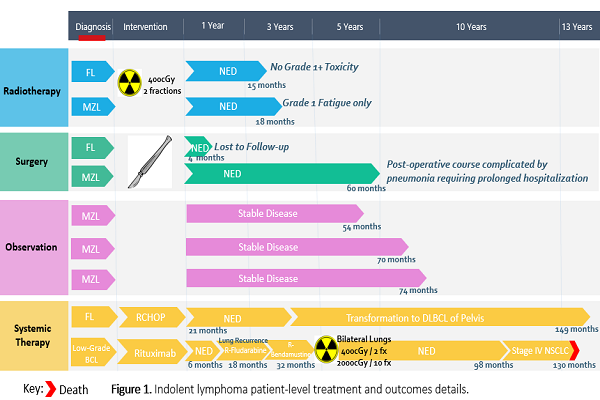
We identified 30 PHL pts within the institutional cohort and 192 pts from comprehensive literature review (Table 1). DLBCL subgroup analysis (n=15) with UVA for OS is listed in Table 2. On MVA for OS, only ECOG score (p=0.02) and Lugano stage (p=0.04) remained significant. Indolent lymphoma subgroup analysis (n=9) with UVA for OS is listed in Table 2 and Figure 1. On MVA for OS, only age remained significant.
| Variable | Institutional Cohort (n=30)
N (%) | Literature Review (n=192)
N (%) |
Gender
Male
Female
Unknown |
16 (53)
14 (47)
-
|
98 (51)
76 (40)
18 (9)
|
Risk Factors
Smoking
Hepatitis C
Hepatitis B
Autoimmune Conditions |
10 (33)
3 (10)
2 (7)
4 (13) |
-
31 (16)
32 (17)
16 (8)
|
Symptoms at Presentation
Incidental Finding
Abdominal Pain
Weight Loss
Jaundice |
9 (30)
8 (27)
6 (20)
3 (10)
|
47 (24)
60 (31)
31 (16)
16 (8) |
ECOG
0
1
2 |
25 (83)
3 (10)
2 (7) | - |
Lugano Staging
I
II
III
IV |
25 (83)
-
3 (10)
2 (7) |
187 (97)
2 (1)
-
3 (2)
|
| Bulky Disease | 6 (20) | 1 (0.5) |
| Nodal Involvement | 3 (10) | 5 (3) |
Treatment Modality
Systemic Therapy
Surgery
Radiation
Observation |
20 (67)
4 (13)
4 (13)
4 (13)
|
96 (50)
69 (36)
10 (5)
11 (6)
|
Vital Status
Alive
Dead
Lost to Follow-up |
17 (57)
8 (27)
5 (17) |
97 (51)
36 (19)
3 (2) |
| Median Follow-up (years) | 6 | 2 |
Table 1. Patient characteristics for institutional and literature review cohorts.
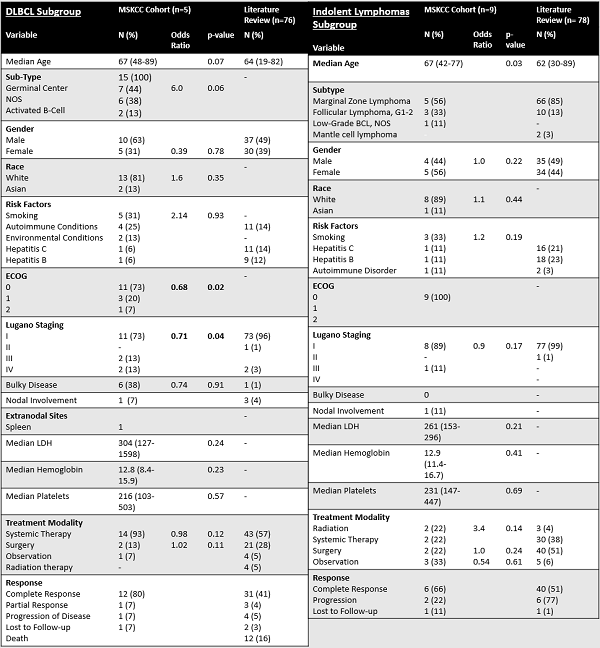
Table 2. Patient characteristics for institutional and literature review cohorts with UVA for OS, by subtype.
Conclusion
PHLs are a rare subtype of NHL without clear
treatment consensus. Primary hepatic DLBCL appears to be treated primarily with
chemotherapy with adequate disease control. For indolent PHL, low-dose RT
appears to achieve good disease control with minimal toxicity. Our RT data is
limited by short follow-up duration of RT pts compared to pts who received
chemotherapy, surgery or observation. However, our results are encouraging for
the use of RT for appropriate patients with indolent PHL.