Advantages of DIBH in IMRT of locally advanced NSCLC systematically investigated with autoplanning
Kristine Fjellanger,
Norway
OC-0287
Abstract
Advantages of DIBH in IMRT of locally advanced NSCLC systematically investigated with autoplanning
Authors: Kristine Fjellanger1,2, Linda Rossi3, Ben J. M. Heijmen3, Helge Egil Seime Pettersen1, Sebastiaan Breedveld3, Inger Marie Sandvik1, Turid Husevåg Sulen1, Liv Bolstad Hysing1,2
1Haukeland University Hospital, Department of Oncology and Medical Physics, Bergen, Norway; 2University of Bergen, Institute of Physics and Technology, Bergen, Norway; 3Erasmus University Medical Center, Department of Radiotherapy, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Studies have found encouraging reproducibility and patient compliance of
deep inspiration breath hold (DIBH) radiotherapy for locally advanced non-small
cell lung cancer (LA-NSCLC). Dosimetric comparisons of DIBH IMRT with free
breathing (FB) IMRT have not been published, and DIBH is not routinely used for
this patient group. This study uses automated multi-criterial planning with
integrated beam angle optimization to systematically compare DIBH IMRT with FB
IMRT, avoiding potential planner bias.
Material and Methods
33 LA-NSCLC patients were prospectively included. One 4DCT and three
DIBH CTs were acquired for each patient. For FB planning, the OARs and GTV were
delineated on the average intensity projection of the 4DCT, and the internal
GTV (IGTV) incorporated the GTV positions on all 4DCT phases. For DIBH
planning, the OARs and GTV were delineated on one DIBH CT, and the IGTV
incorporated the GTV positions on the two repeated DIBH CTs. The CTV was a 5 mm expansion of the IGTV,
adjusted for uninvolved organs, and the PTV was a 5 mm isotropic expansion of
the CTV. A novel in-house system for multi-criterial planning was used to
automatically generate two deliverable 6-beam IMRT plans with optimized beams
angles for each patient, one for FB and one for DIBH. The prescribed dose was
60-70 Gy in 2 Gy fractions. Relevant dose-volume parameters were compared using
the Wilcoxon signed-rank test (p ≤
0.05).
Results
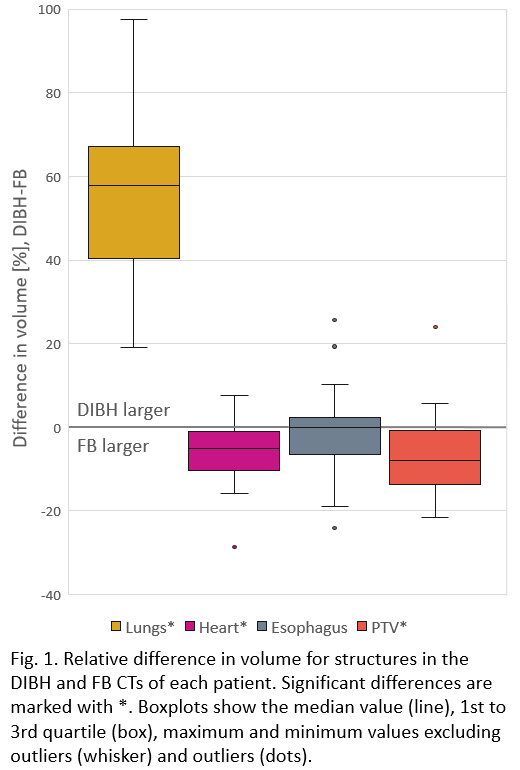
With DIBH, the lung volume increased by on average 54% compared to FB,
while heart and PTV volumes were reduced by 6% and 7% (Fig 1). While DIBH showed
a slightly lower median PTV V95%, all dosimetric parameters for the
lungs, heart and spinal canal were clearly advantageous. For the esophagus, no
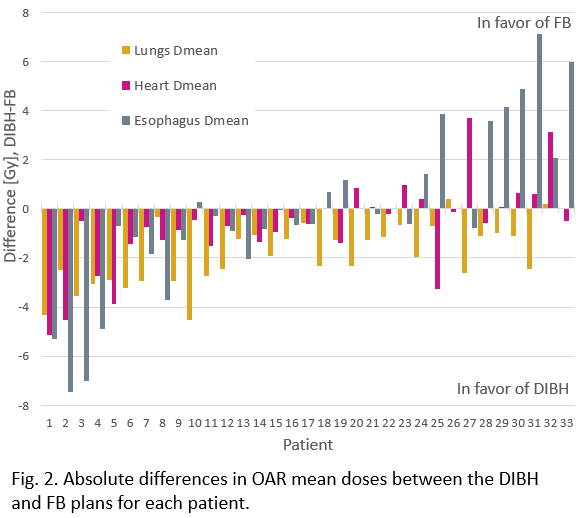
significant differences were found (Table 1). Fig 2 points at large
inter-patient variations in dosimetric differences between FB and DIBH,
especially for the esophagus which could move either towards or away from the
PTV due to DIBH. For 30/33 patients, DIBH resulted in a lower lung Dmean than
FB (>2 Gy for 15 patients), and the heart Dmean was lower for
23/33 patients (>2 Gy for 5 patients).
Table 1: Dose-volume parameters for FB and DIBH.
| FB - Median | FB - IQR | DIBH - Median | DIBH - IQR | p-value |
PTV V95% (%)
| 99.3 | 0.6 | 99.1 | 0.5 | <0.001 |
Lungs Dmean (Gy)
| 15.9 | 4.4 | 13.9 | 3.9 | <0.001
|
Lungs V5Gy (%)
| 58.8 | 17.3 | 54.8 | 15.3 | 0.006 |
Lungs V20Gy (%)
| 25.3 | 9.7 | 24.0 | 7.2 | <0.001
|
Heart Dmean (Gy)
| 8.5 | 7.6 | 7.7 | 6.7 | 0.01 |
Heart V5Gy (%)
| 42.5 | 38.8 | 30.3 | 40.5 | 0.02 |
Heart V30Gy (%)
| 7.8 | 8.9 | 5.7 | 8.4 | 0.02 |
Esophagus Dmean (Gy)
| 19.2 | 12.3 | 19.0 | 6.0 | 0.5 |
Esophagus V20Gy (%)
| 37.6 | 19.4 | 36.9 | 14.4 | 0.1 |
Esophagus V60 Gy (%)
| 4.4 | 13.2 | 4.6 | 10.5 | 0.3 |
Spinal canal Dmax (Gy)
| 44.0 | 10.6 | 42.4 | 14.9 | 0.05 |
Conclusion
For most LA-NSCLC patients, DIBH reduced lung and heart dose compared to
FB. However, dosimetric advantages varied considerably between patients, with individual
patients showing large benefits, others with no or minor benefits, and for a
few patients DIBH was inferior to FB. Automated planning could facilitate
individualized selection between FB and DIBH with virtually zero workload and
no planner bias.