Pareto front analysis for implementing bone marrow sparing VMAT strategy for cervical cancer
Sander Kuipers,
The Netherlands
OC-0130
Abstract
Pareto front analysis for implementing bone marrow sparing VMAT strategy for cervical cancer
Authors: Sander Kuipers1,2, Jérémy Godart2,1, Anouk Corbeau3, Abdul Sharfo1, Sebastiaan Breedveld1, Jan-Willem Mens1, Remi Nout1, Mischa Hoogeman1,2
1Erasmus MC Cancer Institute, Department of Radiotherapy, Rotterdam, The Netherlands; 2HollandPTC, Department of Medical Physics and Informatics, Delft, The Netherlands; 3Leiden University Medical Center, Department of Radiation Oncology, Leiden, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Implementing
bone marrow sparing (BMS) for the treatment of locally advanced cervical cancer
(LACC) with VMAT can reduce the incidence of hematologic toxicity. However,
introducing BMS possibly increases the dose to organs at risk (OARs) in the pelvic region, such
as the bladder and rectum. The aim of this study is to quantify the increase in
bladder and rectum dose when a BMS VMAT strategy is implemented for the
treatment of LACC.
Material and Methods
Twenty patients
with FIGO 2018 stage IB-IVA cervical cancer were selected for analysis. Of the
cohort, 15/20 patients received a simultaneous integrated boost (SIB) to pelvic
lymph nodes and in 2/20 the para-aortic region was included. The bone marrow
was defined as the CT-based whole pelvic bone contour (PB). For every patient, a VMAT base plan with no BMS was created using automated planning. Next, we generated
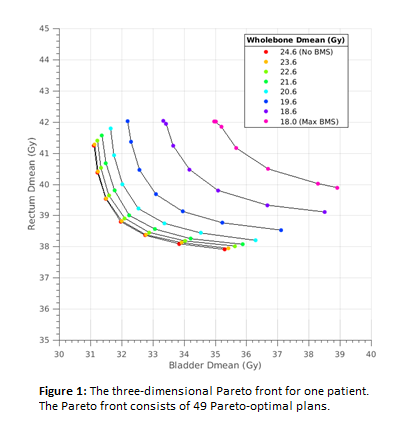
four to eight Pareto fronts per patient depending on the maximum achievable BMS. All plans followed our clinical protocol, which fulfils EMBRACE-II dose
constraints. Every Pareto front consisted of seven Pareto-optimal plans and
showed the trade-off between the mean rectum and bladder doses, while
maintaining a constant mean PB dose. The first Pareto front of a patient had
the same mean PB dose as the base plan, corresponding to 0Gy BMS, and for every
consecutive Pareto front for that patient, we decreased the mean PB dose in
steps of 1Gy until the maximum BMS was reached. The mean dose of the sigmoid,
bowel, kidneys, and duodenum were constrained to a maximum increase of 1Gy
compared to the base plan.
Results
Of the cohort, 19/20
were included for analysis, with convex Pareto fronts for all patients. One
patient was excluded because of large overlap between the bladder and the
target. In total, 798 plans were evaluated. Figure 1 shows the Pareto fronts of
one patient. The average [range] mean dose of PB with no BMS was 22.8 [20.7-26.2]
Gy. When maximum BMS was implemented, the average reduction in mean PB dose was
5.4 [3.0-6.8] Gy resulting in an average mean PB dose of 17.5 [15.8-19.8] Gy.
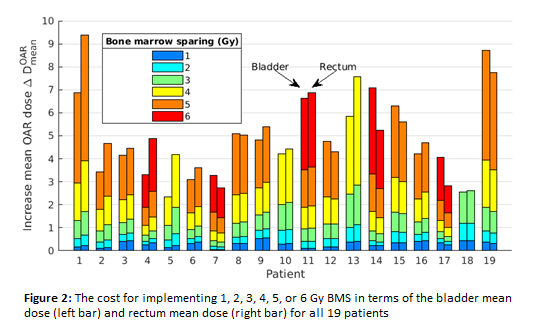
Figure 2 shows the mean increase in the bladder or rectum mean dose for each patient when decreasing the mean PB dose for constant mean dose to other OARs. If <1Gy increase in either the bladder or the rectum mean dose is chosen as a clinically acceptable increase, the PB mean dose can be decreased by >2Gy, >3Gy and >4Gy for 17/19, 5/19, and 1/19 patients, respectively.
Conclusion
The precise trade-off
between the PB, bladder, and rectum dose depends on the patient’s anatomy,
however, all patients showed a similar convex Pareto front. Based on a
comprehensive Pareto front analysis, we conclude that it is possible to decrease
the PB mean dose with 1-4Gy without increasing the dose to other OARs with a
clinically relevant amount (>1Gy). Therefore, we recommend to implement BMS
for the treatment of LACC patients with VMAT.