Prioritising toxicities in NTCP-TCP-based treatment plan optimisation
Hans Paul van der Laan,
The Netherlands
OC-0125
Abstract
Prioritising toxicities in NTCP-TCP-based treatment plan optimisation
Authors: Hans Paul van der Laan1, Arjen van der Schaaf1, Lisa Van den Bosch1, Erik Korevaar1, Stefan Both1, Johannes Langendijk1
1University Medical Center Groningen, Department of Radiation Oncology, Groningen, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
We
recently reported on quality of life (QOL)-guided radiotherapy including
NTCP-based treatment plan optimisation. This method employs NTCP objective
functions, prioritised based on their impact on QOL, instead of conventional
dose-based objective functions for individual organs at risk (OAR). We recently
expanded this method to include simple models for tumour control probability
(TCP) and general plan quality (e.g., hotspot reduction, target dose
homogeneity), allowing for fully automated planning. The aim of this study was
to test the feasibility of this method and to investigate its sensitivity to
the use of different schemes for prioritising toxicities during treatment plan
optimisation.
Material and Methods
Ten
patients, representative of our population receiving definitive (chemo)radiotherapy
for head and neck cancer, were selected for this study. Fully automated VMAT treatment
plans were created using a mix of NTCP and TCP objective functions. TCP
objective functions were based on a PTV D98 ≥ 95% of the prescribed dose. Few fixed
dose-based objectives were added for critical structures. Three automated plans
were created for each patient using different priorities for 20 toxicities including
salivary, swallowing and speech problems, pain and general symptoms. Toxicities
were prioritised according to three schemes: 1) relative impact according to
the published QOL model (weighted toxicity function, with a low priority for salivary
toxicities); 2) identical weights for each toxicity; and 3) prioritised
prevention of salivary toxicities, in which salivary toxicities, swallowing
problems and other toxicities were weighted as 3 : 2 : 1, respectively. For
each patient, the manually created clinical VMAT plan was used as reference. General
plan quality and beam setup was equal or similar for all plans including the
clinical plan. Plans were compared using dose-volume data in combination with NTCP
and QOL using published and validated models.
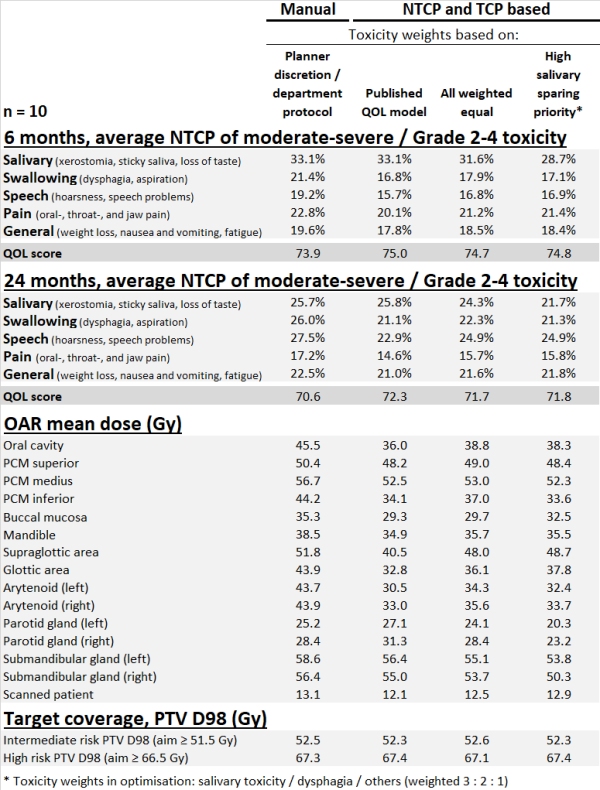
Results
Fully
automated NTCP-TCP-based optimisation consistently resulted in superior plans without
any hotspots. Compared to the clinical plan, all automated plans resulted in a
lower dose in OAR (except for some plans in the parotid glands) and always lower
NTCPs for swallowing, speech, pain and general toxicities. The average QOL
score in the automated plans was always better than in the clinical plans (Table). Automated plans with prioritised prevention of salivary toxicities had the
lowest NTCPs for salivary toxicities, however, at the cost of higher NTCPs for
moderate-to-severe general symptoms such as fatigue. Plans optimised based on
the published QOL model had the best QOL scores.
Conclusion
Automated
NTCP-TCP-based optimisation is feasible and consistently outperforms manually
generated VMAT plans in terms of NTCP and QOL scores. The highest QOL score was
obtained for plans optimized prioritising the toxicities with the highest
relative impact on QOL.