SKIN DOSE STUDY UNDER RPM MARKER BLOCKS IN BREAST TREATMENTS
OC-0124
Abstract
SKIN DOSE STUDY UNDER RPM MARKER BLOCKS IN BREAST TREATMENTS
Authors: Nagore Garcia Apellaniz1, Nuria Jornet1, Jaime Pérez-Alija1, Sonia Olivares1, Cristina Ansón1, Fabia Suriñach1, Pedro Gallego1, Helena Vivancos1, Agustín Ruiz1, Marta Barceló1, Fátima Leo1, Pablo Carrasco1
1Hospital de la Santa Creu i Sant Pau, Servicio de Radiofísica y Radioprotección, Barcelona, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
After including in our routine Varian’s new RPM marker block, we have seen an increase in skin toxicity on the area where it is positioned. The aim of this study is to assess the dosimetric effect of the new Varian marker block.
Material and Methods
Unlike Varian’s previous marker block which has 6 dots, the new one has 4 dots and a posterior wall that is in contact with the patient, potentially increasing the skin dose due to a bolus effect. Phantom measurements were performed for a 6MV X-ray beam from a Varian TrueBeam linac (20x20 cm2 field size and SSD=100) using EBT3 films to check the surface dose with and without the marker block and the attenuation at 3 cm depth beneath. EBT3 films were scanned using an EPSON EXPRESSION 10000XL scanner and FilmQAPro Software. The measured doses were compared to dose calculations on the same phantom setting using Eclipse TPS vs 15.6 (AAA calculation algorithm-grid 0.2 mm).
A total of 55 breast patients were included in a prospective study to assess skin dose in vivo with EBT3 films of 2x2 cm2 inside sleeves of low-density polyethylene of 50 µm thickness. Films were positioned medially inside the internal tangential beam under the marker block, if any. Different techniques with the 6 dots, 4 dots and no marker block were included. Most treatments only use 6MV X-ray beams, 10 MV X-rays are used only for low weighted beams in some 3D-CRT plans. Prescribed dose per fraction was 2.67 Gy. We used the Mann–Whitney U test to analyse the skin dose difference by technique and marker block.
Results
The phantom measurements showed a 3-fold surface dose increase under the block and the attenuation 3 cm beneath it was on average 1.3%, reaching 4.5% under the markers. These results agreed with TPS calculations.
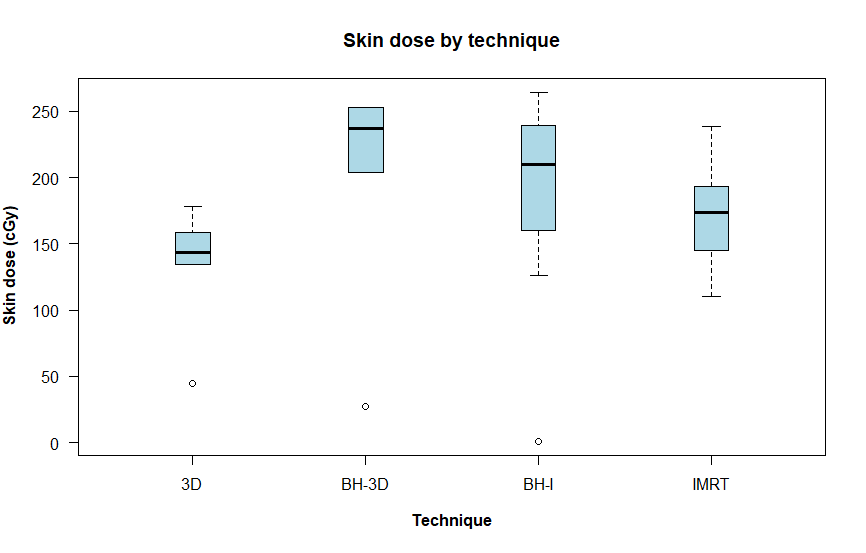
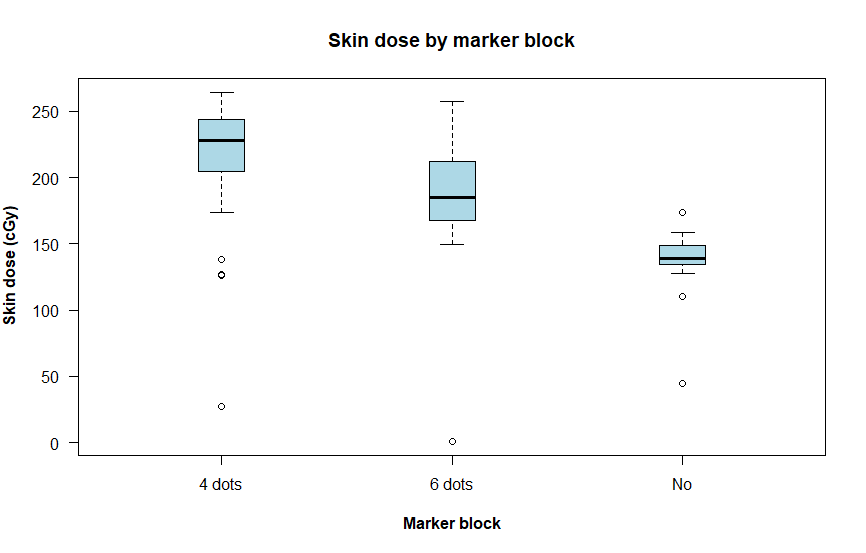
Figure 1 shows the in vivo skin dose measurements for the patients included in the study stratified per technique. The skin dose is higher for BH techniques irrespective of the marker block used and technique (IMRT or 3D-CRT), showing significance (p=0.032) for IMRT vs IMRT-BH (both using respiratory control). The results also indicate a significant increase of skin dose when using any of the marker blocks (p<0.002) but the difference was not significant when comparing the 4 dots marker block with 6 dots marker block (p=0.057) (Fig. 2).
Conclusion
For the breast patients included in the study, we have found that skin dose is higher for BH than for IMRT techniques. When using RPM marker blocks we found an increase in the skin dose higher for the 4 dots marker blocks. These results are consistent with phantom measurements. In order not to increase skin toxicity the marker block should be placed outside the treatment fields. If not possible, the marker block should be included in the body contour for dose calculation. The use of EBT3 films for in vivo dosimetry is useful to monitor skin dose.