Results: One hundred
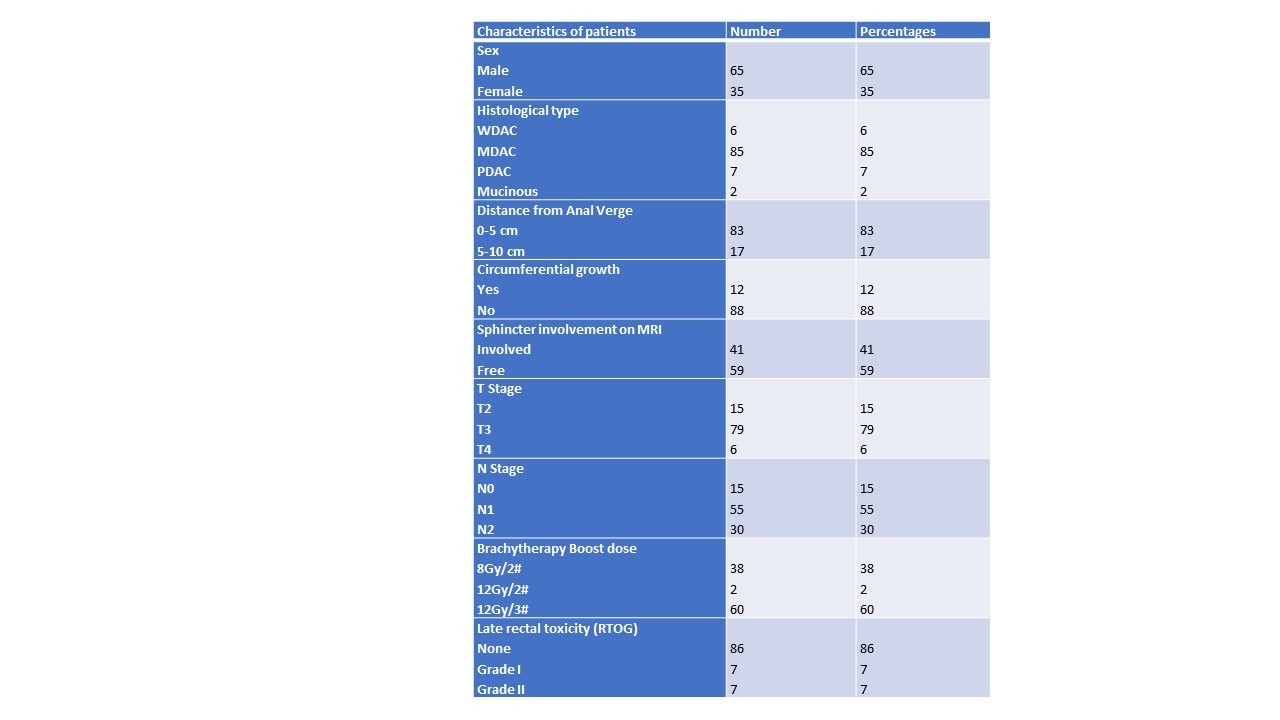
patients treated between December 2017 to April 2021receiving endorectal
brachytherapy post NACTRT were identified. External beam radiotherapy was given
to a dose of 45-55Gy (median 50Gy) in conventional
fractionation with concurrent Capecitabine, followed by endorectal
brachytherapy 8-12Gy in 2-3 (median 12Gy/3) fractions. Brachytherapy was performed at a
median time of 2 (range 1-4) weeks post last fraction of EBRT.
The overall nCR/cCR rate was
50% (20 nCR, 30 cCR and 50 PR). Of the 50 patients with cCR/nCR, 7 were
unwilling for W&W and underwent surgical resection (5 had pCR, 1 pN1,
1-pT3N0) and the rest 43 patients were kept on observation. Fifty patients
having partial response underwent TME
At a median follow-up of 26
months (IQR 14-38 months) 5 (11.6%) patients on W&W had local regrowth (2 also
with distant metastasis). All except 1 were surgically salvaged.
Overall organ preservation
rate was 39%. The only factor influencing cCR/nCR was baseline T and N stage.
Of the 15 T2 ttumors 12(80%) had cCR whereas of the 85 T3 tumors 38 (45%) had
cCR/nCR (p_0.02). Similarly absence of mesorectal nodes was associated with
higher cCR/nCR rate (73% vs 46%, p_0.04)
Late rectal toxicity was
observed in 12 (25%) patients with 6 having Grade 1 and another 6 Grade 2. DFS.
Overall survival being 100%
Overall 8(8%) developed
distant metastasis 4 from the WW group and 4 from PR group.
Conclusion: Endorectal
brachytherapy is a safe and feasible technique to enhance complete response,
reducing local regrowth and thus improving organ preservation for distal rectal
cancers.